Case presentation: Breast abscess
Obiozor A.A, MBBS, FWACS,1 Obiozor A.C, B. Pharm NIG2
Abstract
Background: Breast abscess is a localized collection of pus within the breast tissue, often caused by bacterial infection like staphylococcus and salmonella organisms. It typically arises as a complication of mastitis. Breast abscesses, although more prevalent in lactating women, can occur in non-lactating women like in this case presentation and can pose a diagnostic challenge. Predisposing factors includes trauma to the breast, breast surgery, or preexisting conditions like diabetes or immunosuppression. Clinically, a breast abscess presents with symptoms such as localized pain, swelling, redness, and sometimes fever and malaise. Diagnosis, is primarily based on clinical examination, laboratory tests and imaging studies, such as mammography, ultrasound in order to confirm the presence and extent of the abscess. Treatment involves antibiotics to address the infection and drainage of the abscess, either through needle aspiration or surgical intervention, to remove the pus and alleviate symptoms. Prompt treatment is crucial to prevent complications such as sepsis or chronic infection. The prognosis is generally good with timely and appropriate management, although recurrence can occur.
Methods: This case report presents the radiological evaluation of a breast abscess in a 25-year-old non-lactating woman who presented in a radio-diagnostic centre in Umuahia with complaints of breast swelling, breast pain and fever for one week. Consent was taken from the patient and clinical examination revealed a small skin ulceration over the right breast mass, febrile patient with temperature of 38 degrees centigrade, laboratory test revealed elevated leucocytes with white blood cell count of (15,000/µL) and neutrophilia., fine needle aspiration biopsy/culture revealed staphylococcus aureus, imaging modalities, including mammography revealed a radio-dense mass in the right breast middle ring. Ultrasound revealed a Hypoechoic mass with thick wall, internal echoes and posterior acoustic enhancement with surrounding area of increased vascularity in the upper outer quadrant middle ring which is consistent with an abscess cavity. The diagnosis of breast abscess was confirmed, and appropriate treatment was administered.
Conclusion: This report aims to underscore the crucial role of radiological assessment, laboratory tests in diagnosing breast abscesses, thereby facilitating prompt and effective management.
Keywords: Breast abscess, Laboratory tests, Fine needle aspiration biopsy, Ultrasonography, Mammography
Introduction
Breast abscesses are localized collections of pus within the breast tissue, often resulting from bacterial infections. While typically associated with lactation, these abscesses can also occur in non-lactating women due to various factors such as trauma, surgery, or underlying health conditions. This case report details the radiological evaluation of a breast abscess in a 25-year-old non lactating woman, emphasizing the importance of imaging and laboratory tests in the diagnosis and management of this condition.
Case Presentation
A 25-year-old non gravid woman presented to the clinic with acute onset of right breast pain, swelling, redness and skin ulceration over the right breast. She reported no history of recent trauma, surgery, or lactation. On physical examination, a tender, erythematous mass was palpable in the upper outer quadrant of the right breast. Focused examination revealed a small skin ulceration over the right breast mass, Patient was febrile with temperature of 38 degrees centigrade, laboratory test revealed elevated leucocytes with white blood cell count of (15,000/µL) and neutrophilia, fine needle aspiration biopsy/culture revealed staphylococcus aureus, imaging modalities, including mammography revealed a radio-dense mass in the right breast middle ring, while Ultrasound showed a Hypoechoic mass with thick wall, internal echoes and posterior acoustic enhancement with surrounding area of increased vascularity in the upper outer quadrant middle ring which is consistent with an abscess cavity. The diagnosis of breast abscess was confirmed, and appropriate treatment was administered.

Fig 1. Picture of breast abscess in the right upper outer quadrant middle ring when patient was on no medication
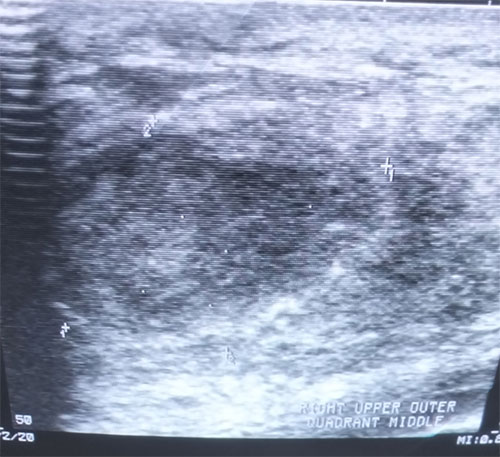
Fig 2. Ultrasound picture of the right breast abscess with thick wall
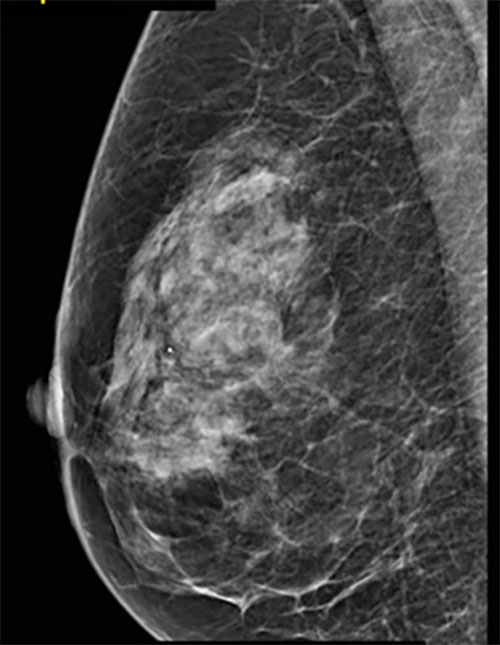
Fig 3. Mammogram of Right breast abscess medio-lateral view (MLO)
Treatment involved ultrasound-guided aspiration of the abscess. About 50 mL of purulent fluid was aspirated. She was placed on intravenous antibiotic therapy with Augmentin 1.2g eight hourly for 3days in the referred hospital as an outpatient then followed with tablet Augmentin 625mg 12hrly for 1week, patient retroviral status was negative and her HB was 13g/dl. Supportive care with analgesic and warm compression to the affected area helped patient to respond well to treatment, with resolution of symptoms and no recurrence at the three-month follow-up. Consideration of incision and drainage would have been done if aspiration was not effective or if the abscess reoccurred.
Discussion
This case underscores the importance of considering breast abscesses in the differential diagnosis for women presenting with breast pain and swelling, irrespective of their lactation status. Radiological imaging, particularly ultrasound, plays a pivotal role in confirming the diagnosis and guiding the treatment approach. Early intervention is crucial to prevent complications and ensure favorable outcomes.
It is acknowledged that the highest incidence of breast abscess occurs in lactating women1. It was argued by Adler2 that one cause of this infection is fissuring of the nipple from which bacteria gain entry into the periglandular tissue, another cause being “missed or delayed feeding or attempted weaning, which leads to milk stasis and subsequent bacterial overgrowth and infection.” Undoubtedly, these antecedents are prevalent in West African community. Hughes3 remarked on a recent school of thought that proposed “fibrocystic disease to be a ‘non-disease. Because it is a common, benign, and hormone-driven condition that doesn't lead to serious health issues and typically requires no treatment beyond symptom management. The early presentation for treatment in this case highlights the significance and potential severity of such symptoms. Does breast abscess contribute to the work load of surgeons all over the world? Cox’s colleagues4 were impressed by the fact that patients with either a lump, discharge from the nipple or pain in the breast represent a considerable work load at a general surgical clinic in England. In the study done in South Africa by Hayley Irusen et al5. They stated that all abscesses in the incision and drainage (I&D) group were successfully treated. Moreover, out of 434 biopsies in a Saudi Arabian hospital, Altaf6 saw cases of breast abscess. Furthermore, from the United States, Ekland and Zeigler7 reported on patients with abscess in the non-lactating breast. In their view, incision and drainage or excision results in satisfactory resolution of the inflammation. Such satisfaction must have been felt in this developing community. It is well for worldwide research to be undertaken on this type of breast disease. In this context, it is interesting that in a recent Nigerian tabulation8, the mean age of cases of breast abscess was 39 years which is not in consistent with the age of this patient. Another possible reason for attendance to clinics is the awareness of breast cancer. Elsewhere, it was shown that public awareness was manifested in cases of breast fibroadenoma among teenagers in the community9. Although there is evidence that some Nigerian women show persistent extreme denial when suffering from breast cancer10, the rising temporal trend evident in the present study is consistent with prevailing enlightened awareness.
References
- Raju GC, Naraynsingh V, Jankey N. Post-menopausal breast abscess. Postgrad Med 132 J, 1986; 62: 1017-1018.
- Adler HL. Breast infection. In: Meakins JL, ed. Surgical Infections. New York; Scientific American, Inc.; 1994: 287. 137
- Hughes LE. Classification of benign breast disorders. Br Med Bull, 1991; 47: 251- 138 257. 139
- Cox PJ, Li MKW, Ellis H. Spectrum of breast disease in outpatient surgical practice. 140 J Roy Soc Med, 1982; 75: 857-859. 141
- Hayley irusen, Anke C. Rohwer, D wilhelm steyn, Taryn young and Cochrane Pregnancy and Childbirth Group National library of medicine Treatments for breast abscesses in breastfeeding women Cochrane Database Syst Rev. 2015; 2015(8): CD010490. https://doi.org/10.1002/14651858.CD010490
- Altaf FJ. Patterns of breast diseases: King Khalid National Guard Hospital 142 experience. Ann Saudi Med, 2001; 21: 239-241. 143
- Ekland DA, Zeigler MG. Abscess in the non-lactating breast. Arch Surg, 1973; 107: 144 398-401. 145
- Akhator A. Benign breast masses in Nigeria. Nig J Surg Sci, 2007; 17: 105-108. 146
- Onuigbo WIB. Breast fibroadenoma in teenage females. Turk J Pediat, 2003; 45: 147 326-328. 148
- Onuigbo WIB, Mbanaso AU. Persistent extreme denial in five nurses suffering from 149 breast cancer. J Coll Med, 2006; 11: 5-7.