Impalement injury to the head with intact neurology following spontaneous Dane gun explosion: Two case reports and review of the literature
Abubakar Yahaya, Aliyu M. Koko
Abstract
Introduction: Impalement brain injury is a complex brain trauma resulting from unusual mechanisms, especially in areas bedevilled by civil unrest.
Objective: To describe the successful management of impalement head injury in our centre.
Case description: A 22 and 18-year-old man presented with altered consciousness following head trauma by a recoiled metallic part of the Dane gun. Clinical and radiological evaluations were in keeping with the impalement head injury. They were successfully managed by foreign object retrieval, antibiotics, and anticonvulsants and discharged home with no neurological deficits.
Conclusion: The two cases of impalement head injury had remarkable recovery following prompt surgical removal, antibiotics and wound care.
Keywords: impalement head injury, Dane gun, traumatic brain injury, craniotomy, craniectomy
Introduction
Impalement injuries are among penetrating injuries to the brain, caused by a retained, blunt or sharp object that perforates the brain along its longitudinal axis producing a wound track corresponding to its length of penetration.1 Impalement brain injury is rare and the management could be tasking as a result of neural tissue damage, risk of brain infections and abscess, seizure and long-term disability.2
Most of the impalement craniocerebral injuries are accidental,3 and varying objects such as knives, nails, brushes, screwdrivers, wood, metallic parts of Dane guns and pencils have been reported in the literature.5,6,8,10 Most patients with a penetrating brain injury (PBI) die before arriving at a hospital or emergency department, and survivors are at a high risk of morbidity from haemorrhage and severe cranial injuries.9
However, some cases with good neurological outcomes have been reported.2 Most of the studies on impalement head injuries in literature were case reports and case series as such, there is a paucity of standardised management protocols that will minimize disability and death from this dreaded form of head injury. Therefore, this report aims to unfold our experience with the management of two cases of impalement head injuries following the explosion of a Dane gun.
Case 1
A 22-year male vigilante presented with an 8-hour history of loss of consciousness and, a metallic part of the Dane gun impaled on his head. The Gun was said to be loaded with gunpowder and exploded, the object flew backwards and retained into his right temporal and the right occipital region. There was associated brain evisceration and bleeding. No seizures, and no other injuries elsewhere. Examination revealed a young man, restless, and pale. Central nervous system examination revealed a GCS of 10(E2V3 M5). Left Pupil was 3mm in size and reactive to light, while the right pupil couldnÆt be assessed due to periorbital oedema. Moves all the limbs equally. Brain CT showed an impaled metallic object in the right frontotemporal and parieto-occipital lobes, with comminuted fractures, contusions and surrounding oedema. He was resuscitated with intravenous fluid, blood, tetanus prophylaxis, antibiotics (moxifloxacin and metronidazole), and phenobarbitone injections. A Craniotomy was performed to remove the foreign body. A T-shaped skin incision was made, the flap was reflected, the bone flap was raised, then a C-shaped durotomy was made, and the object was cleaned with povidone-iodine and removed gradually in an antegrade direction ( from temporal to occipital). Haemostasis was achieved. Augmented duroplasty using pericranium was carried out. The patientÆs postoperative course was uneventful. He was discharged without any neurological deficits and counselled regular follow-up visits.
Case 2
An 18-year-old man presented with a 4-hour history of impaling part of the Dane gun on his head, the gun was said to be loaded and exploded, and the object recoiled and retained into his right parietal region. He lapsed into unconsciousness and bled from the wound. No seizures, no other injuries elsewhere. On general examination revealed a young man, restless, and pale. His GCS was 11, Pupils were 3mm sluggishly reactive to light bilaterally. Moves all the limbs equally. Brain CT showed an impaled metallic part of Dane gun in the right parietal region, comminuted fractures, contusions and surrounding oedema. He was resuscitated with intravenous fluid, blood, tetanus prophylaxis and antibiotics (moxifloxacin and metronidazole) administered. A craniectomy was performed to retrieve the foreign body. Hemostasis was secured. Augmented duroplasty was done. The patient had remarkable postoperative recovery and was discharged home to see a neurosurgery outpatient clinic for follow-up.
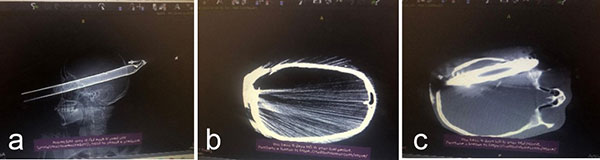
Figure 1 is a Brain CT scan which shows a scout film, b-comminuted occipital fractures, and a Pneumocephalus c-bone window that shows an impaled object.
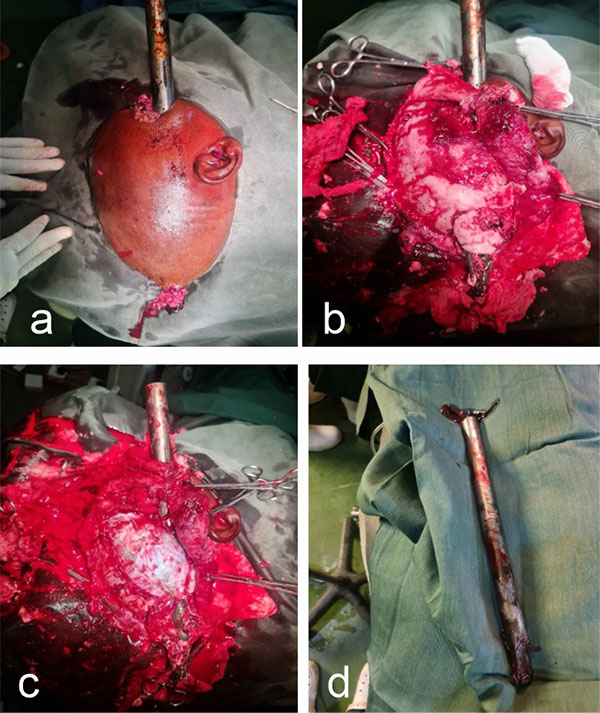
Figure 2 is an intraoperative picture which shows a-Op-site was cleaned and draped b-Skin flap was raised and fractures visualised. C-exposed dura visualised d-retrieved object.
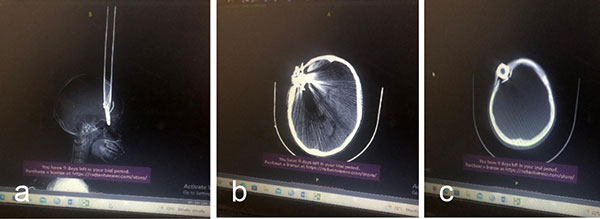
Figure 3 brain CT scan shows A-scout with impaled object B-fractures, contusion, pneumocephalus. C-Bone window with impaled object
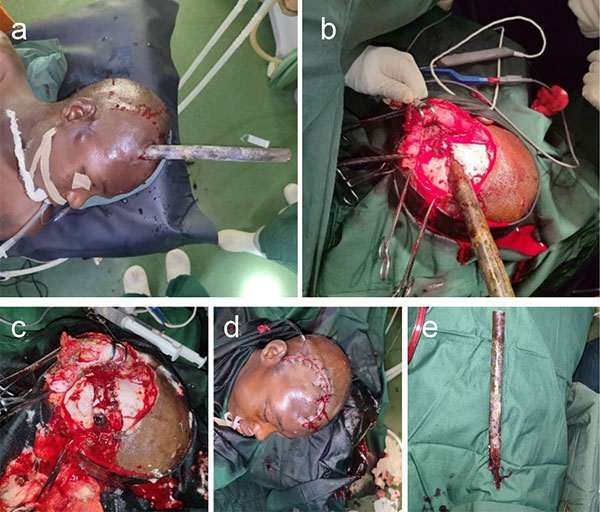
Figure 4- Intraoperative pictures which show A-Op-site draped. B-Skin flap raised and fracture visible. C-craniectomy and retrieval of impaled objects. D-skin closure and subgaleal drain placed e-retrieved object.

Figure 5 shows an example of a Dane gun used in our society taped
Discussion
We experienced rare cases of impalement brain injury caused by a metal bar of Dane gun with a complicated shape, prompt and proper care confers good neurological outcomes. Early recognition, careful debridement and judicious antibiotic therapy, anticonvulsants, and Tetanus prophylaxis can limit or prevent complications in the management of these patients.3 Removal of impaling objects at the site of injury is strongly discouraged because can lead to haemorrhage, and the outcome is better in a well-designed procedure in a neurosurgical theatre.4-7 It was worth observing that the rescuers, not being trained health personnel, left the impaling object intact. The two cases presented were young males (18 and 22 years old), untrained in handling guns, so more prone to accidental discharge and explosion. Most of the patients reported in the literature were in their third decade of life,1,2,8 these findings corroborated with our findings. Males are twice as likely as females to suffer from these injuries.1,8 Also, all our two patients were males, maybe because generally head injuries are more common in males due to their being involved in more risky outdoor activities and defending their family than females. In some patients, a part of the impaling object can pierce through the opposite side.3 This is found in our first case that the impaling object pierces the opposite site, however, in our second case it didnÆt perforate the other side. So the kinetic energy conducted in the first case was higher than in the second case.
A previous study reported that patients with higher GCS scores had better outcomes than those with lower scores.6,8 The above findings were in keeping with our patients' higher GCS on admission (10 and 11) for the first and second cases respectively, which explains their better outcomes. It is advocated to administer antibiotics, and anticonvulsants in the literature because of the high risk of infection and seizures.6 Our patients were given anticonvulsants at presentation to reduce the risk of seizure, which can cause secondary brain injury and worsen the patient outcomes, antibiotics and Tetanus toxoids can reduce the risk of CNS infection and tetanus respectively.
In our first case, the impaled metallic Dane gun was retrieved by craniotomy, durotomy and augmented duroplasty using pericranium. We offered him craniotomy because the object was deeply seated, with brain contusion, and diffuse brain oedema, aimed at reduction in intracranial pressure, this was in keeping with the previous case report that offered their clients craniotomy,2 and contrary to those that did craniectomy to retrieve the impaled object.1,8 However, for our second case, craniectomy was done because the object was found to be more superficially and vertically oriented so the bone adjacent to the metal was nibbled to let it loose and then impaled object then retrieved, this was also favoured by some authors.1,8 We record a superficial site infection in both cases which were managed with wound care and antibiotics therapy. The first case, in addition, developed a CSF leak from the wound which was treated non-operatively with acetazolamide. The second case had cranioplasty 6 months later due to a skull defect after the infection had subsided. Due to the aforementioned criminal activities, people in different cities of Northern Nigeria, are making local guns for self-defence. Factors that lead to gunshot explosion or accidental discharge may include careless handling or by individuals untrained in gun safety. Sometimes, a firearm may discharge accidentally due to a mechanical defect or malfunction, even when handled correctly, or it can occur when firearms are not kept safely. Like in our index case it appeared none of the measures were put in place. Their local gun was overloaded with gunpowder. So it easily exploded and recoiled.
Conclusion
We managed a rare form of impalement brain injuries. Therefore, prompt resuscitation, antibiotics, Tetanus prophylaxis anticonvulsant therapies and timely surgical intervention are recommended for better outcomes. The enlightenment of the community via social media and other means of communication as well as control of rampant gun handling by the government will minimize the occurrence of these complex brain injuries.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Yusuf AS, Mahmud MR, Alfin JD, Adeleke NA. Clinical presentation and outcome of impalement cranio-cerebral injuriesŚa case series.JWACS.2017; 7(2):112¢23.
- Wataru T, Kaho Y, Akira E, Yasuhiro O. A Case of Impalement Brain Injury That Could Achieve Good Neurological Outcome by Introducing Early Sedation and Immobilization Strategy. Case Rep Ophthalmol Med. 2018;3025717.
- Kazim SF, Shamim MS, Tahir MZ, Enam SA, Waheed S. Management of penetrating brain injury. J Emerg Trauma Shock.2011;4(3):395-402.
- Kim S.W, Youn S.K, Kim J.T, Cho S.H, Kim Y.H, and Hwang K.T, ōManagement of an Unusual Craniofacial Impalement Injury by a Metallic Foreign Body,ö The Journ of Craniofacial Surgery.2012; 23:2, 140¢146.
- Binitie OP. Impalement head injuries. JWACS. 2017; 2: X¢Xii.
- Binitie OP, Shilong DJ, Ugwu BT, Ekedigwe JE, Oyeniran OO, Adighije PF et al. Impalement head injury with a serrated meat knife. JWACS. 2012; 2:67¢74.
- Chika TA, Mathew EO. Management of a nail impalement injury to the brain in a non-neurosurgical Centre: a case report and review of the literature. IntJ Surg Case Rep. 2016; 19:115¢8.
- Koko AM, Lasseini A. Impalement brain injury: report of five consecutive clinical cases. Egyptian J of Neurosurg.2020; 35(5):1-6.
- Williams N, Bulstrode C, OÆConnell P, editors. Bailey and LoveÆs Short Practice of Surgery. Boca Raton: CRC Press; 2013
- Akhiwu BI, Adoga AS, Binitie OP, Ani CC, Iweagwu M, Adetutu O, Ureme T, George DD, Didamson PD, Oseni-Momodu E, Ugwu BT. Impalement head injury with a spear. J West Afr Coll Surg. 2016 04 - 06;6(2):113¢124
- Langlois JA, Kegler SR, Butler JA, Gotsch KE, Johnson RL, Reichard AA, et al. Traumatic Brain Injury-Related Hospital Discharges: Results from a 14-State Surveillance System, 1997. Washington, DC, USA: Centers for Disease Control and Prevention NCfIPaC, MMWR Surveillance Summaries; 2003. p. 1-18