Prevalence of Probable Sarcopenia and Associated Lifestyle Factors among Elderly Retired Nigerian Soldiers
Fidelis O. Ajuonuma,FWACP,1 Benjamin Y. Ibrahim,FWACP,2 Zubairu HD,FWACP,3 Natie N. Butawa,FWACP4
Abstract
Background: Probable Sarcopenia is the age-related decline in muscle strength. It is a pre-sarcopenic state that is amenable to lifestyle modification. This study aimed to determine the prevalence of probable sarcopenia and the modifiable lifestyle factors associated with it among the elderly retired Nigerian soldiers.
Methodology: The study was a hospital based cross sectional study. Eligible participants were recruited for the study using a systematic random sampling method. A total of 327 participants were recruited for the study. Data on demographic characteristics and lifestyle risk factors were obtained. Probable sarcopenia was diagnosed by low grip strength. Frequency of the risk factors were determined, Chi square test was used to test for the association between the risk factors and probable sarcopenia. Multivariable logistic regression analysis was used to identify the independent predictive risk factor associated with probable sarcopenia among the participants.
Result: The proportion of the study participants found to have probable sarcopenia was 63.3%. Lack of regular physical exercise was the only lifestyle risk factor that showed significant association with probable sarcopenia (P < 0.05). Multivariable logistic regression analysis showed that lack of regular physical exercise is an independent predictor of probable sarcopenia among the participants.
Conclusion: There is a high prevalence of probable sarcopenia among elderly retired Nigerian soldiers. Routine screening by healthcare providers with hand-held dynamometer is recommended for its early identification and adoption of regular physical exercise as a lifestyle after retirement can prevent its progression.
Key words: Probable Sarcopenia, Elderly, Retired Soldiers, Exercise, Nigeria.
Introduction
Sarcopenia is a significant geriatric giant that causes mobility disorders, increased risk of falls with fractures, impaired ability to perform activities of daily living, disabilities, loss of independence and increased risk of death as a result of the progressive loss of muscle strength, mass and function with ageing.1 Operationally, sarcopenia has been defined by both low muscle mass and strength, but recent evidence suggests that muscle strength alone is a better predictor of these adverse outcomes.2 This has led to the concept of probable or possible sarcopenia, defined as low muscle strength with normal muscle mass.3,4 Identifying individuals in this pre-sarcopenic state is crucial for early intervention to prevent the progression to full sarcopenia.5 Two major international guidelines are used to screen at-risk older adults for probable sarcopenia: the European Working Group on Sarcopenia in Older People (EWGSOP2, 2018) and the Asia Working Group for Sarcopenia (AWGS, 2019).4 Both guidelines recommend measuring hand grip strength with a dynamometer but suggest different cut-off values: The EWGSOP2 recommended <27kg and <16kg for men and women respectively while AWGS recommended <28kg and <18kg respectively for men and women.2,4 Given population differences, other studies outside Europe and Asia have used normative cut-values derived from young adults within their populations.6,7 The prevalence of probable sarcopenia in Nigeria and Africa has not been determined. However, studies in other regions have reported varying prevalence rates. A European study among community-dwelling older Swiss adults found a prevalence of 26.3% in women and 28.0% in men.3 In Asia, a study among community-dwelling older Korean adults reported prevalence rates of 20.1% in men and 29.2% in women.8 A recent Peruvian study estimated the prevalence of probable sarcopenia to be 22.7% using EWGSOP2 criteria and 27.8% using AWGS criteria.9
The progression of sarcopenia in the older adults is significantly associated with modifiable lifestyle factors such as various aspects of nutrition, physical activity, exercise, alcohol intake, and tobacco use.10 Long-term cigarette smoking has been linked to sarcopenia through various mechanisms.11,12 Alcohol consumption, particularly heavy drinking, has been identified as a risk factor for low muscle mass and strength, as demonstrated in a study from Zanan province, China.13 Lack of exercise and low physical activity are critical underlying factors in the development and progression of sarcopenia.14 Stress is another important risk factor in geriatrics which affects muscle mass and strength and should be managed efficiently through counselling, yoga or meditation to prevent further muscle loss and disability.15 Given the modifiability of these lifestyle factors, early identification and intervention are essential in managing the elderly to delay the onset and prevent the progression of sarcopenia. Probable sarcopenia identifies at-risk elderly individuals who would benefit from lifestyle modifications. This study aimed to assess the prevalence of probable sarcopenia and its association with lifestyle factors among elderly retired Nigerian soldiers, a unique and previously unstudied population.
Methods
This cross-sectional analytical study was carried out at the Retirees Unit of the General Out-Patient Clinic of 44 Nigerian Army Reference Hospital Kaduna (44NARHK), the sole Military Reference Hospital in the North-Western geo-political zone of Nigeria. It provides primary, secondary and tertiary care to both serving and retired military personnel and their families as well as the general public living within and outside Kaduna state.
The study population comprised of all the elderly retired soldiers aged (60 years and above) both males and females who attended the retirees unit between November, 2022 and March, 2023. The sample size was calculated using the Kish Leslie formula for cross-sectional studies.16 A sarcopenia prevalence of 30.7% from our pilot study in a sister military facility was used in this calculation.
Sample size: n = z2 pq/d2
Where
n = sample size when population is > 10,000
Z = Z-score was set at 1.96 which corresponds to 95% confidence level.
p = Proportion in the target population estimated to have particular characteristics (retired elderly soldiers with sarcopenia)
q = 1-p
Prevalence rate of 30.7% was used as the proportion of retired elderly soldiers with sarcopenia.
p = 0.307
q = 1.0 – p = 1.0 – 0.307 = 0.693
d = (the degree of accuracy) = 5% = 0.05
Therefore n = (1.96)2 (0.307) (0.693)/(0.05)2 = 326.8 = 327 (minimum sample size).
The study participants included all those who consented to the study. Exclusion criteria were severely sick, those with deformity, disability or frank psychosis. A total number of 327 participants were recruited for this study following a systematic sampling method. Pre-tested, semi-structured interviewer administered questionnaire was used to obtain the demographic and lifestyle characteristics data from the participants.
Diagnosis of Probable Sarcopenia
The operational definition of probable sarcopenia followed the revised consensus criteria of the European Working Group on Sarcopenia in Older People (EWGSOP2).4 This definition identifies probable sarcopenia based on low muscle strength alone. Cut-off points were derived as recommended by the consensus criteria from a consenting cohort of young serving soldiers aged 20-35 years (15 males and 15 females), based on -2 standard deviations (SD) from the mean. For this study population, low muscle strength was defined as =34.49 kg for males and =22.64 kg for females.
Measurement of Muscle Strength- The muscle strength of the study participants were assessed by their hand grip strength as recommended by the EWGSOP2. The grip strength has been found to correlate moderately with strength in other body compartments.4 This measurement was performed with a digital hand-held dynamometer (Camry Electronic Hand Dynamometer Model: EH 101). The participant while seated comfortably and arms well rested on the chair arms was asked to squeeze the handle of the dynamometer with his or her dominant hand as strongest as he or she could. The reading on the display in kilogram was recorded as the grip strength.
Ethical Consideration- Ethical clearance for this study was obtained from the ethical and research committee of 44 NARHK (44NARHK/G1/300/20). The participants gave written consent after been duly informed about the study. The data handling was done with utmost confidentiality.
Data Analysis- The statistical package for social sciences SPSS (version 23.0, IBM Corp., Armonk, New York) was used for the data entry, cleaning and analysis. There were no missing data. Descriptive statistics was summarised in tables. Qualitative variables were expressed in proportions or frequency and quantitative variables were illustrated by means and standard deviations. The association between categorical variables was tested with chi-square test while logistic regression analysis was used to determine the independent predictors of probable sarcopenia among the identified significant variables. Confidence level was set at 95% and P-value of < 0.05 was considered as significant.
Results
The study participants included 327 elderly retired soldiers whose age range was (60-103) years. The mean age was 73.18 ±7.45 years. They comprised 317 (96.9%) males and 10 (3.1%) females. The assessed lifestyle factors showed that majority 246 (75.2%) had no smoking history, 186 (56.9%) were having regular exercise, and only 126 (38.5%) had history of alcohol ingestion. They all had various methods of stress management but majority 223 (68.2%) used Resting. None of the participants used illicit substances. Majority 235 (71.9%) had cordial relationship with their neighbours, only 10 (3.1%) did not get along well. Probable sarcopenia was diagnosed in 207 (63.3%) of the participants. (Table 1) The Chi-square test showed that only exercise had a significant association with probable sarcopenia [?2= 8.063, p= 0.005] (Table 2). Logistic regression analysis showed that those with no exercise history had an odds ratio (OR) of 1.929 at 95% CI [1.223 – 3.045] for developing probable sarcopenia (Table 3)
Table 1: Demographic and Lifestyle Characteristics of the Study Participants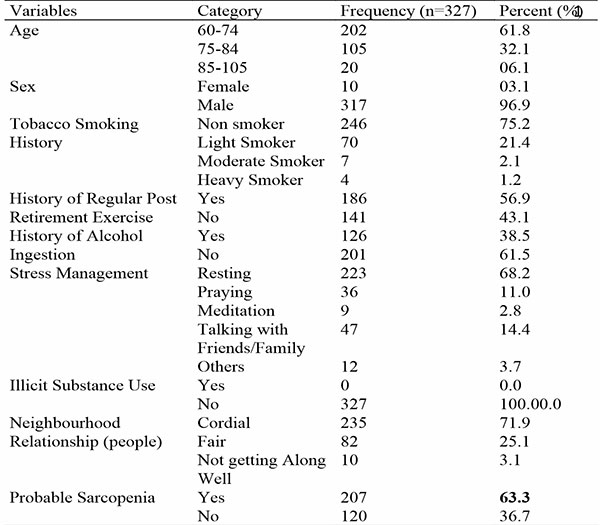
Table 2: Association of Lifestyle Characteristics with Probable Sarcopenia among the Study Participants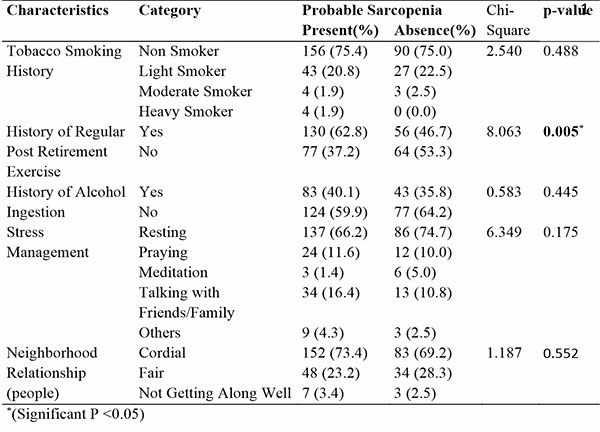
Table 3: Logistic Regression Analysis of Factor Significantly Associated with Probable Sarcopenia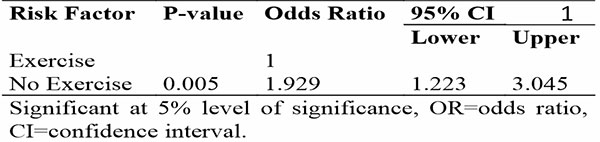
Discussion
This study assessed 327 elderly retired soldiers who are community-dwelling with mean age of 73.18±7.45 years and found a probable sarcopenia prevalence of 63.3% among them. This shows that this unique elderly Nigerian population have majority of them in this pathologic pre-sarcopenic state. While data from African studies are scarce, some studies have reported even much higher prevalence. Franzon et al. reported a prevalence of 73% in very old Swedish men.17 Another study in Portugal using Ishii`s formula, found prevalence of 73.5% among hospitalized geriatric patients.18 A Chinese study with similarly aged older adults found a prevalence of 48.06%.4 These studies, like ours, measured grip strength with a hand dynamometer. Variability in prevalence can be attributed to population differences and the mean age of study participants, grouped into youngest-old (60-74), middle-old (75-84), and oldest-old (85 and older).19,20 Some studies found lower prevalence rates: Su et al. in Japan21 found 14.5% while Kim et al. in Korea8 found 20.1% in men and 29.2% in women. The high prevalence of probable sarcopenia in this study implies that 63.3% of elderly retired Nigerian soldiers are at risk. Sarcopenia is associated with disabilities, loss of independence, and death, highlighting the importance of prevention, early diagnosis, and treatment. Among the lifestyle factors assessed, only exercise showed a significant relationship with probable sarcopenia. In this study, it was found that elderly retired soldiers with no history of regular exercise had a 93% higher chance of developing probable sarcopenia compared to those who exercised regularly. This finding aligns with other studies. Hämäläinen et al. found that the lowest levels of self-reported physical activity were associated with increased probable sarcopenia risk.22 Wu et al. found that moderate to high physical activity protected against sarcopenia in Taiwanese older adults.23 Another study on physical activity and sarcopenia incidence found that moderate-high physical activity significantly reduced the likelihood of sarcopenia.24 Regular exercise increases the level of physical activity which have been found to have an anabolic effect especially on ageing muscles as it enhances its sensitivity to amino acids involved in muscle protein synthesis.25 Increasing the muscle protein synthesis not only prevents loss of mass but also increases the contractile tissues of the muscle as well as its performance. Thus exercise is a countermeasure to the ageing effect on muscles; a lifestyle elderly retired soldiers must be encouraged to pursue with vigour.26,27 This study found contrary to expectation that almost half of the participants (43.1%) were not engaged in regular physical exercise despite its significant health benefits. The reasons for this will be a subject for further research. A recent systematic review came up with three broad themes of factors that influence older people’s participation in regular physical exercise which include lack of capability, lack of opportunity and lack of motivation.28 It is therefore pertinent to recommend to Nigerian legion, the need to institute regular exercise programme for her members for a healthy ageing.
Limitation: This study was limited by its hospital-based nature, which may not reflect the true prevalence of probable sarcopenia among other retirees who did not visit the hospital. Additionally, the cross-sectional design precluded establishing causality between probable sarcopenia and the lifestyle risk factors assessed.
Conclusion: Probable sarcopenia is highly prevalent among elderly retired Nigerian soldiers, with a significant association with lack of regular physical exercise. Lack of regular physical exercise was identified as an independent predictor. It is recommended that structured regular fitness exercises for military personnel continue post-retirement for healthier aging.
Competing Interests: The authors have no known duality of interest.
Funding: There was no external funding.
Authors` Contributions:
- FO and BY conceived the study.
- FO performed the data collection.
- BY supervised the data collection.
- FO, NN, HD analysed the data.
- FO drafted the manuscript.
- HD and BY critically revised the manuscript and all the authors have read and agreed to the final manuscript.
Acknowledgements: The support and commitment of the commander/CMD of 44NARHK is highly appreciated.
Data Availability Statement: “Data available upon reasonable request, subject to Nigerian Army institutional review board approval”
References
- Cruz-Jentoft AJ, Pierre Baeyens J, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(1):412–23.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyčre O, Cederholm T, et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing. 2019; 48(1):16–31.
- Wearing J, Konings P, De Bie RA, Stokes M, De Bruin ED. Prevalence of probable sarcopenia in community-dwelling older Swiss people- A cross-sectional study. BMC Geriatr. 2020;20(1):1–8.
- Yao J, Wang Y, Yang L, Ren M, Li L, Wang H. Original research: Prevalence of possible sarcopenia in community-dwelling older Chinese adults: a cross-sectional study. BMJ Open. 2022;12(12):1–7.
- Trierweiler H, Kisielewicz G, Jonasson TH, Petterle RR, Moreira CA, Borba VZC. Sarcopenia: A chronic complication of type 2 diabetes mellitus. Diabetol Metab Syndr. 2018;10(1):1–9.
- Huemer MT, Kluttig A, Fischer B, Ahrens W, Castell S, Ebert N, et al. Grip strength values and cut-off points based on over 200,000 adults of the German National Cohort - a comparison to the EWGSOP2 cut-off points. Age Ageing. 2023;52(1):1–10.
- Adebusoye L, Ogunbode A, Olowookere O, Ajayi S, Ladipo M. Factors associated with sarcopenia among older patients attending a geriatric clinic in Nigeria. Niger J Clin Pract . 2018;21(4):443–50.
- Kim M, Won CW. Sarcopenia in Korean Community-Dwelling Adults Aged 70 Years and Older: Application of Screening and Diagnostic Tools From the Asian Working Group for Sarcopenia 2019 Update. J Am Med Dir Assoc. 2020;21(6):752–8.
- Flores-Flores O, Zevallos-Morales A, Pollard SL, Checkley W, Siddharthan T, Hurst JR, et al. Sarcopenia and sarcopenic obesity among community-dwelling Peruvian adults: A cross-sectional study. PLoS One. 2024;19(4):1–13.
- Rom O, Kaisari S, Aizenbud D, Reznick AZ. Lifestyle and Sarcopenia—Etiology, Prevention, and Treatment. Rambam Maimonides Med J. 2012;3(4):1–12.
- Rom O, Kaisari S, Aizenbud D, Reznick AZ. Sarcopenia and smoking: A possible cellular model of cigarette smoke effects on muscle protein breakdown. Ann N Y Acad Sci. 2012;1259(1):47–53.
- Petersen AMW, Magkos F, Atherton P, Selby A, Smith K, Rennie MJ, et al. Smoking impairs muscle protein synthesis and increases the expression of myostatin and MAFbx in muscle. Am J Physiol - Endocrinol Metab. 2007;293(3):843–8.
- Zhai J, Ma B, Qin J, Lyu Q, Khatun P, Liang R, et al. Alcohol consumption patterns and the risk of sarcopenia: a population-based cross-sectional study among chinese women and men from Henan province. BMC Public Health. 2022;22(1):1894–901.
- Fribereger E, Sieber C, Pfeifer K. Physical activity, exercise, and sarcopenia - Future challenges. Wiener Medizinische Wochenschrift. 2011;161(17–18):416–25.
- Poornima KN, Karthick N, Sitalakshmi R. Study of the effect of stress on skeletal muscle function in geriatrics. J Clin Diagnostic Res [Internet]. 2014;8(1):8–9.
- Serdar CC, Cihan M, Yücel D, Serdar MA. Sample size, power and effect size revisited: Simplified and practical approachin pre-clinical, clinical and laboratory studies. Biochem Medica. 2021;31(1):1–27.
- Franzon K, Zethelius B, Cederholm T, Kilander L. The impact of muscle function, muscle mass and sarcopenia on independent ageing in very old Swedish men. BMC Geriatr. 2019;19(1):153–62.
- Cavalheiro A, Afonso S, Silva M, Ramalhăo N, Machado J, Magalhăes S. Evaluation of Probable Sarcopenia’s Prevalence in Hospitalized Geriatric Patients Using Ishii’s Score. Cureus. 2023;15(11):1–8.
- Lee SB, Oh JH, Park JH, Choi SP, Wee JH. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin Exp Emerg Med. 2018;5(4):249–55.
- Escourrou E, Laurent S, Leroux J, Oustric S, Gardette V. The shift from old age to very old age: an analysis of the perception of aging among older people. BMC Prim Care. 2022;23(3):1–10.
- Su Y, Hirayama K, Han TF, Izutsu M, Yuki M. Sarcopenia prevalence and risk factors among japanese community dwelling older adults living in a snow-covered city according to EWGSOP2. J Clin Med. 2019;8(3):291–304.
- Hämäläinen O, Tirkkonen A, Savikangas T, Alén M, Sipilä S, Hautala A. Low physical activity is a risk factor for sarcopenia: a cross-sectional analysis of two exercise trials on community-dwelling older adults. BMC Geriatr. 2024;24(1):212–25.
- Ko YC, Chie WC, Wu TY, Ho CY, Yu WR. A cross-sectional study about the relationship between physical activity and sarcopenia in Taiwanese older adults. Sci Reports 2021 111. 2021;11(1):1–9.
- Mijnarends DM, Koster A, Schols JMGA, Meijers JMM, Halfens RJG, Gudnason V, et al. Physical activity and incidence of sarcopenia: the population-based AGES—Reykjavik Study. Age Ageing. 2016;45(5):614–20.
- Yang Y, Breen L, Burd NA, Hector AJ, Churchward-Venne TA, Josse AR, et al. Resistance exercise enhances myofibrillar protein synthesis with graded intakes of whey protein in older men. Br J Nutr. 2012;108(10):1780–8.
- Garatachea N, Pareja-Galeano H, Sanchis-Gomar F, Santos-Lozano A, Fiuza-Luces C, Morán M, et al. Exercise Attenuates the Major Hallmarks of Aging. Rejuvenation Res. 2015;18(1):57–80.
- Distefano G, Goodpaster BH. Effects of Exercise and Aging on Skeletal Muscle. Cold Spring Harb Perspect Med. 2018;8(3):1–16.
- Meredith SJ, Cox NJ, Ibrahim K, Higson J, McNiff J, Mitchell S, et al. Factors that Influence Older Adults' Participation in Physical Activity: A Systematic Review of Qualitative Studies. Age and Ageing. 2023; 52(8):1-15