The prevalence of sexual dysfunction, anxiety and depression in pre-dialysis chronic kidney disease patients in Uyo, Nigeria
Effiong E. Akpan, Aniema IA. Udo, Victor A. Umoh
Abstract
Background: Chronic kidney disease (CKD) is a progressive condition that spans years or even decades. It is therefore associated with comorbidities as well as other complications among which include erectile dysfunction (ED), anxiety, and depression.
Method: This was a cross- sectional descriptive study involving 54 male pre-dialysis patients seen in the renal clinic of the University of Uyo Teaching Hospital, Uyo, Nigeria. The history of erectile dysfunction (ED) was taken using the abridge five-item version of the 15-item well-validated International Index of Erection Function (IIEF-5) questionnaire. Anxiety and depression were evaluated using the simple hospital anxiety and depression scale (HADS) screening tool.
Results: Fifty-four (54) pre-dialysis male patients were recruited, aged between 26 and 67 with a mean age of 49.65 ±8.37. Only 1(1.87%) was single, 53(98.13%) were married. The prevalence of erectile dysfunction was 81.5%. Erectile dysfunction had a significant association with depression and anxiety. Respondents had Anxiety, with a Borderline of 7(29%), clinical casenesss 31(57.4%) against normal of 16 (29.6%). While 35(64.8%) had depression, borderline 15(27.8%), caseness of 20(37%) against normal 19(35.2%). Anxiety and depression had a strong association with erectile dysfunction p= 0.02 and p= 0.01 respectively.
Conclusion: There is a high prevalence of ED, anxiety, and depression among pre-dialysis male patients. ED is strongly associated with anxiety and depression.
There is a need always to evaluate our male CKD patients for ED, anxiety, and depression and possibly consider treatment in severe cases.
Keywords: Erectile dysfunction, chronic kidney disease, depression, anxiety.
Introduction
Background of the study: Chronic kidney disease(CKD) is a progressive condition that spans years or even decades. It is therefore associated with comorbidities as well as other complications among which include erectile dysfunction (ED), anxiety and depression1-2. Depression and, anxiety have been found to be the primary mental health disorders among patients with CKD3-4. These comorbidities and complications generally affect and worsen both morbidity and mortality. In addition, some of the complications like erectile dysfunction, anxiety, and depression have a negative impact on quality of life.
Depression alone is said to be second only to hypertension as a comorbid condition in patients with end-stage renal disease (ESRD)5. Depression and anxiety disorders are often underestimated and underdiagnosed in CKD patients6. This is further compounded by uremia3. Depression in CKD patients is also associated with poor quality of life.1
Erectile dysfunction (ED) is defined as the inability to attain and/or maintain penile erection sufficient for satisfactory sexual performance. It is now a common condition and approximately 150 million males worldwide are estimated to suffer from ED7. This number is projected to double by the year 20258. The common risk factors for ED include age, smoking hypertension, diabetes mellitus, and hyperlipidemia with CKD recently added to this list of risk factors2. This association is not surprising as most of the common causes of CKD are by themselves causes of ED. Diagnosis and treatment of ED in chronic kidney disease patients post a great challenge.
The prevalence of ED in CKD patients has been reported to be about 70% on average9. One study reported a prevalence rate of 91.6% among those just starting dialysis10. Sexual dysfunction in CKD is multi-factorial and affected by a several physiological conditions such as hypothalamic-pituitary–gonadal axis and vascular supply, while psychological factors include fatigue, stress and, depression. Co-morbid conditions like diabetes, hypertension and, obesity also contribute. Erectile dysfunction among CKD patients may be further compounded by drugs commonly used to manage its complications such as antihypertensives and diuretics. Sexual dysfunction has been reported as increasing in frequency as renal function declines before renal replacement therapy11. A study has identified ED as an early symptom of chronic renal failure12.
The high prevalence of ED in patients with CKD significantly affects their quality of life. Despite this, little or no attention given to these patients in our practice. The goal of treating patients with chronic kidney disease should include improvement in the quality of life and this should take into account improvement in their sexual life. Sexual dysfunction according to Finkelstein et al13 is associated with anxiety, loss of self-confidence and self-esteem, marital discord, and depression, all of which contribute to impaired quality of life.
This study is therefore designed to examine the prevalence of ED, depression and, anxiety among our CKD patients and to determine any association among these condition.
Subjects and method: This is a cross-sectional descriptive study involving male pre-dialysis patients.
Their socio-demographic data were recorded using a structured questionnaire. A thorough medical history including a history of hypertension, diabetes, and drugs was recorded. All participants were examined by Nephrologists. Weight and height were measured using Seca weighing scale and blood pressure was taken using Accuson’s sphygmomanometer after 10 minutes rest. An average of two readings was taken as the blood pressure of the patient.
Erectile dysfunction was assessed using the abridge five-item version of the 15-item well-validated International Index of Erection Function (IIEF-5) questionnaire14. This is a 15-question multi-dimensional, self-administered questionnaire that has been found useful in the clinical assessment of erectile dysfunction. The survey assesses five domains. 1. Erectile function. 2. Orgasmic function. 3. Sexual desire. 4. Intercourse satisfaction and 5. Overall satisfaction. Erectile function is assess using questions 1-5 and question 15. Questions 1-5 has a score of 0-5 each, while question 15 have a score of 1-5. The International Index of Erection Function (IIEF-5) classified ED severity into the following 5 categories based on their scores; severe (5-7), moderate (8-11), mild to moderate (12-16), mild (17-21), and no erectile dysfunction (22- 25).
Anxiety and depression were evaluated and recorded using a simple hospital anxiety and depression scale (HADS)15 screening tool. This scale has been validated and found to be very useful in the assessment of anxiety and depression15-16.The scale consists of 7 questions each for anxiety and depression. Each question is scored 0-3 with a total score of 21 for each condition. A score of 0-7 in the respective subclass is considered normal, with 8-10 borderline and 11 or over indicating clinical caseness. Clinical caseness is a more severe illness that needs clinical intervention.
Male CKD patients aged 18 years and above who met the inclusion criteria were recruited for the study.
Patients on sexual enhancement medications, those with a history of stroke, spinal cord injury, varicocele, and those who refused consent were excluded from the study.
Data handling: Statistical Package for Social Sciences (SPSS) version 23.0 – SPSS Inc., Chicago, IL. U.S.A. was used for analysis. Categorical data was presented as frequencies (and percentages) while continuous data was presented as means (and standard deviation). The prevalence of ED was presented as a percentage (and 95% confidence interval). Chi-square test was used in testing the relationship between two variables. Multivariate analysis was used to determine the association between variables. All p-values = 0.05 were deemed statistically significant.
Ethical Clearance: Ethical clearance was sought and obtained from the University of Uyo Teaching Hospital ethical committee
Consent: Written consent was obtained from all participants. Those who refused consent were excluded from the study.
Results
Table 1: Sociodemographic data of Respondents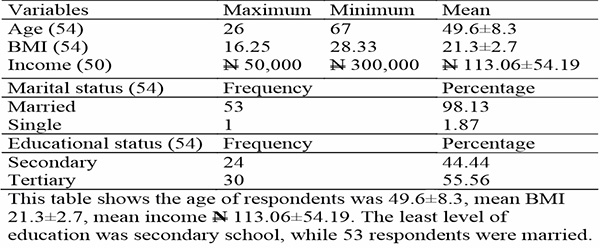
Table 1 showed the sociodemgraphic data of the respondents. Fifty four (54) pre-dialysis patients were recruited, aged 26 and 67 with the mean age of 49.7 ±8.4.
Their body basal index was between 16.3 and 28.3(±2.7). The average monthly income of the respondents was N 113, 6.00±54,191.00 naira.
Only 1(1.9%) was single, 53(98.1%) were married. While 24(44.4%) of the respondents had secondary education, and those with tertiary education were 30(55.6%).
Table 2: Prevalence of erectile dysfunction among the respondents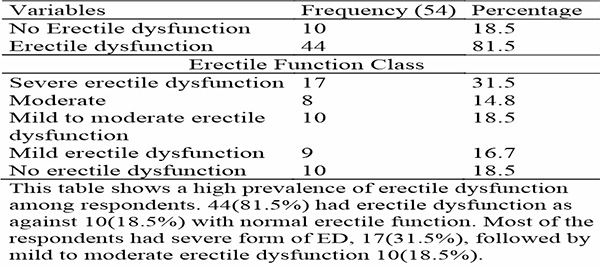
Table 2 shows that 44(81.5%) of the respondents had erectile dysfunction, out of which 17(31.5%) had severe erectile dysfunction, 8(14.8%) had moderate ED, 15(27.8%) had mild to moderate ED and, 3(5.6%) had mild ED respectively, while 10(18.5%) had no erectile dysfunction.
Table 3: Prevalence of anxiety and depression among the respondents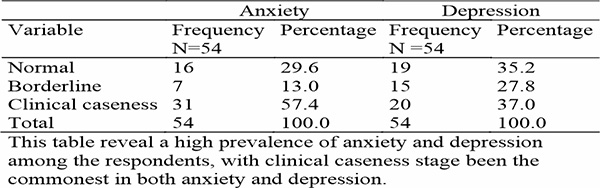
Table 3 shows a high prevalence of depression and anxiety among respondents. For Anxiety, Borderline was 7(13%), caseness 31(57.4%) against normal of 16 (29.6%). While depression had borderline of 15(27.8%), caseness 20(37%) against normal 19(35.2%).
Table 4: Association between erectile dysfunction with depression and anxiety among the Respondents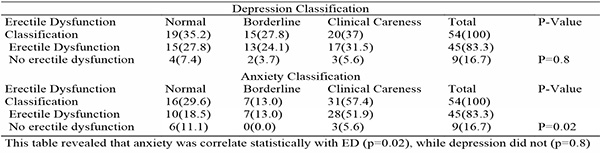
In univariate analysis (table 4), anxiety had a strong association with erectile dysfunction (p= 0.02) depression however didn’t have a significant association with ED (p=0.8).
Table 5: Relationship between erectile dysfunction and causes of CKD
Table 5 shows that ED did not also correlate with causes of CKD among the Respondent.
Table 6: Relationship between erectile dysfunction and age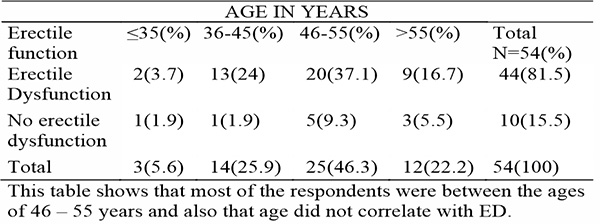
Table 6 shows that ED did not also correlate with age of the Respondent.
Tables 7: Showing the relationship between monthly income with anxiety, depression and ED.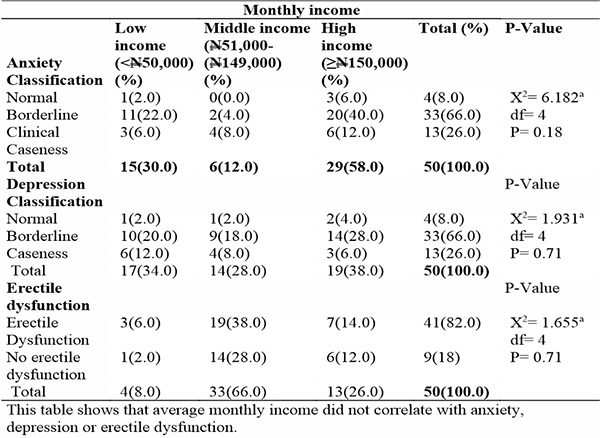
Table 7 shows that Level of income did not correlate with depression, anxiety or ED.
Table 8: Multivariate analysis showing the relationship between ED and co-factors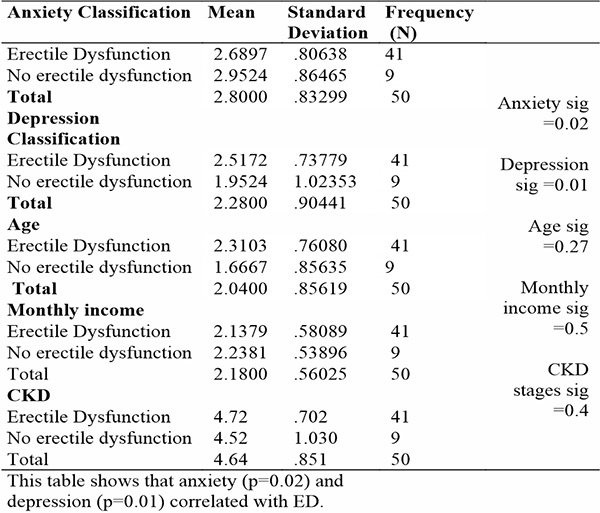
Table 8 shows that anxiety and depression correlate with in ED in multivariate analysis.
Discussion
This study revealed a high prevalence of erectile dysfunction (ED) among male, pre-dialysis chronic kidney disease (CKD) patients. This is erectile dysfunction in CKD patients is dependent on the coordination of multiple systems, including vascular, neurological, psychological, and hormonal factors.
Erectile dysfunction in CKD is a common issue that is difficult to diagnose and treat. Prevalence estimates of sexual dysfunction range from 9% in pre-dialysis to 70% in dialysis patients of either sex9,17.
In our study the prevalence of erectile dysfunction was 81.5%. This finding is higher than that of the general population. In the United States general population, the prevalence of ED in men is 31%18. Idung et al19 found a prevalence of 41.5% in the Niger Delta region of Nigeria. Conversely the study by Abu et al showed a prevalence of 66.4%20. Apart from the fact that Abu et al20 study was not on CKD patients, their respondents were older aged up to 76 years, whereas the oldest respondent in our study was 64 years.
Another study on the prevalence of erectile dysfunction among chronic failure on conservative management also observed a prevalence rate of 81.5% among their older subjects, aligning with our finding in this study21. However, their younger subjects aged 21 to 60 years had a lower ED prevalence of 66.7%. This observation was lower than our findings because our studied population was mainly middle-aged with oldest respondent being 64 years old. This age range may have contributed to the lack of statistical significance between age and erectile dysfunction in this study. Another study on patients on conservative treatment of chronic renal failure found a prevalence rate of 71.02%22. Although lower than our 81.5%, it still supports the fact ED is common in pre-dialysis patients and calls for early evaluation and treatment for the overall well-being of chronic kidney disease patients.
Although age, diabetes, and hypertension are known to affect sexual function,19-23 we found no significant correlation with ED in CKD patients. This may be because erectile dysfunction in CKD patients are multi-factorial including psychological factors such as financial stress, and fear of possible commencement dialysis, stress, malnutrition, systemic illness like diabetes, and hypertension , sex hormones disturbances, hyperthyroidism, anemia, uremia, autonomic neuropathy, and medications24-26. Uremia alone has been shown to account for 79% of erectile dysfunction25. It is believed that the treatment of erectile dysfunction in patients with CKD is largely underutilized due to these multifaceted causes Navaneethan et al9.
We also assessed the prevalence of anxiety and depression among CKD patients and their association with erectile dysfunction. We found a high prevalence of anxiety and depression among pre-dialysis chronic kidney male patients. The prevalence of anxiety was 70.4%, while depression was 64.8%. This is consistent with several studies on the prevalence of anxiety and depression among chronic kidney patients26,27. This may be due to various factors particularly psychological distress, which is common among CKD patient6,28. These mood disorders may be a result of multiple pathophysiological, psychological, and socioeconomic stressors imposed by chronic kidney disease28.
Sexual dysfunction is associated with anxiety and depression resulting in loss of self-confidence and self-esteem, all of which contribute to impaired quality of life13. This study revealed a strong association between anxiety and erectile dysfunction. This is not surprising as psychological factors such as anxiety and depression have been shown in several studies to be one of the major contributors to ED in CKD patients2,6,9. Sexual function also largely depends on the patient’s mood29.
Conclusion: Erectile dysfunction, anxiety, and depression are common among CKD patients. There is an association between anxiety and depression with ED in CKD. For a better quality of life, CKD patients should be routinely evaluated for these conditions.
Limitation: This study is limited by a relatively small sample size. Further research with a larger sample size is suggested.
Competing Interest: We declare that we have no conflict of interest.
References
- Rebollo Rubio A, Morales Asencio JM, Eugenia Pons Raventos M. Depression, anxiety and health-related quality of life amongst patients who are starting dialysis treatment. J Ren Care. 2017 Jun;43(2):73–82.
- Cerqueira J, Moraes M, Glina S. Erectile dysfunction: prevalence and associated variables in patients with chronic renal failure. Int J Impot Res. 2002 Apr;14(2):65–71.
- Cukor D, Coplan J, Brown C, Friedman S, Cromwell-Smith A, Peterson RA, et al. Depression and anxiety in urban hemodialysis patients. Clin J Am Soc Nephrol CJASN. 2007 May;2(3):484–90.
- Azegbeobor J, Lasebikan V. Depression and Disability in Chronic Kidney Disease in Nigeria: A Case-Control Study. Int Neuropsychiatr Dis J. 2016 Jan 10;7(2):1–13.
- United States Renal Data System Annual Data Report 2004 | GHDx [Internet]. [cited 2024 Jul 5]. Available from: https://ghdx.healthdata.org/record/united-states-renal-data-system-annual-data-report-2004
- Kimmel PL, Peterson RA. PSYCHOSOCIAL FACTORS IN PATIENTS WITH CHRONIC KIDNEY DISEASE: Depression in End-Stage Renal Disease Patients Treated With Hemodialysis: Tools, Correlates, Outcomes, and Needs. Semin Dial. 2005 Mar 4;18(2):91–7.
- Seftel AD, Sun P, Swindle R. The Prevalence of Hypertension, Hyperlipidemia, Diabetes Mellitus And Depression In Men With Erectile Dysfunction. J Urol. 2004 Jun;171(6 Part 1):2341–5.
- Aytaç, Mckinlay, Krane. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999 Jul;84(1):50–6.
- Navaneethan SD, Vecchio M, Johnson DW, Saglimbene V, Graziano G, Pellegrini F, et al. Prevalence and Correlates of Self-Reported Sexual Dysfunction in CKD: A Meta-analysis of Observational Studies. Am J Kidney Dis. 2010 Oct;56(4):670–85.
- Gorsane I, Amri N, Younsi F, Helal I, Kheder A. Erectile dysfunction in hemodialysis patients. Saudi J Kidney Dis Transplant. 2016 Jan 1;27:23.
- Ayub W, Fletcher S. End-stage renal disease and erectile dysfunction. Is there any hope? Nephrol Dial Transplant. 2000 Oct 1;15(10):1525–8.
- Cirakoglu A, Yuce A, Benli E, Kasko Arici Y, Dugeroglu H, Ogreden E. Is erectile dysfunction an early clinical symptom of chronic kidney disease? Aging Male. 2021 Jan 1;24(1):24–8.
- Finkelstein FO, Shirani S, Wuerth D, Finkelstein SH. Therapy Insight: sexual dysfunction in patients with chronic kidney disease. Nat Clin Pract Nephrol. 2007 Apr;3(4):200–7.
- Rosen RC, Seftel AD. Validated questionnaires for assessing sexual dysfunction and BPH/LUTS: solidifying the common pathophysiologic link. Int J Impot Res. 2008 Dec;20 Suppl 3:S27-32.
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983 Jun;67(6):361–70.
- Michopoulos I, Douzenis A, Kalkavoura C, Christodoulou C, Michalopoulou P, Kalemi G, et al. Hospital Anxiety and Depression Scale (HADS): validation in a Greek general hospital sample. Ann Gen Psychiatry. 2008 Mar 6;7:4.
- Vecchio M, Palmer SC, Tonelli M, Johnson DW, Strippoli GFM. Depression and sexual dysfunction in chronic kidney disease: a narrative review of the evidence in areas of significant unmet need. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc - Eur Ren Assoc. 2012 Sep;27(9):3420–8.
- Laumann EO, Paik A, Rosen RC. Sexual Dysfunction in the United States: Prevalence and Predictors. JAMA. 1999 Feb 10;281(6):537.
- Idung A, Abasiubong F, Ukott I, Udoh S, Unadike B. Prevalence and risk factors of erectile dysfunction in Niger delta region, Nigeria. Afr Health Sci. 2012 Jun;12(2):160–5.
- Abu S, Atim T, Ripiye NR. Prevalence of Erectile Dysfunction and Awareness of Its Treatment in Abuja, Nigeria. Int J Trop Dis Health. 2019 Jul 23;1–10.
- Mesquita JFP, Ramos TF, Mesquita FP, Netto JMB, Bastos MG, de Figueiredo AA. Prevalence of erectile dysfunction in chronic renal disease patients on conservative treatment. Clinics. 2012 Feb 1;67(2):181–3.
- Costa MR, Ponciano VC, Costa TR, De Oliveira AM, Gomes CP, De Oliveira EC. Prevalence and factors associated with erectile dysfunction in patients with chronic kidney disease on conservative treatment. Int J Impot Res. 2017 Nov;29(6):219–24.
- Oyelade BO, Jemilohun AC, Aderibigbe SA. Prevalence of erectile dysfunction and possible risk factors among men of South-Western Nigeria: a population based study. Pan Afr Med J [Internet]. 2016 Aug 6 [cited 2024 Aug 16];24(124). Available from: https://www.panafrican-med-journal.com//content/article/24/124/full
- Palmer BF. Sexual dysfunction in uremia. J Am Soc Nephrol JASN. 1999 Jun;10(6):1381–8.
- Rodger RS, Fletcher K, Dewar JH, Genner D, McHugh M, Wilkinson R, et al. Prevalence and pathogenesis of impotence in one hundred uremic men. Uremia Invest. 1984 1985;8(2):89–96.
- Cukor D, Coplan J, Brown C, Peterson RA, Kimmel PL. Course of depression and anxiety diagnosis in patients treated with hemodialysis: a 16-month follow-up. Clin J Am Soc Nephrol CJASN. 2008 Nov;3(6):1752–8.
- Huang CW, Wee PH, Low LL, Koong YLA, Htay H, Fan Q, et al. Prevalence and risk factors for elevated anxiety symptoms and anxiety disorders in chronic kidney disease: A systematic review and meta-analysis. Gen Hosp Psychiatry. 2021;69:27–40.
- Zalai D, Szeifert L, Novak M. Psychological Distress and Depression in Patients with Chronic Kidney Disease. Semin Dial. 2012;25(4):428–38.
- Suzuki E, Nishimatsu H, Oba S, Takahashi M, Homma Y. Chronic kidney disease and erectile dysfunction. World J Nephrol. 2014 Nov 6;3(4):220–9.