Assessment of the acceptance and implementation of child survival strategies among mothers in some selected communities in south-south Nigeria
*Peters GE1, Ekpenyong AU1, Moffat BE2, Akpan-Idiok PA1
Abstract
Objective: The aim of this study was to assess the acceptance and implementation of child survival strategies through knowledge and practices among mothers in some selected communities in south-south Nigeria.
Method: A descriptive survey method was used for the study and Rivers state which is in South-South Nigeria was randomly selected for the pilot study. The study was conducted between September 2021 and August 2023 and a sample size of Six Hundred respondents were randomly selected from the three senatorial districts of Rivers State. The instrument used for data collection was researchers’ constructed questionnaire with 17 items grouped into A and B. Section A contained information on demographic data of the respondents while section B focused on the Knowledge, practices and factors that influenced the acceptance and implementation of child survival strategies among mothers in some selected Local Government Areas in Rivers state. Data was analysed using descriptive statistics of percentages in frequency and tables.
Results: The results of the findings showed a high level of knowledge (100%) and its components like skilled child birth attendance (92%), exclusive breastfeeding (83%), immunization (96%) and family planning (78.5%). Also majority of the mothers actually practiced the components of child survival strategies in this study, except family planning services (16%) despite being in the peak of their reproductive years and already having between four to six children. Other factors such as the attitude of the health workers and educational background of mothers were also identified as barriers to the practice of child survival strategies.
Conclusion: It was therefore recommended amongst others that government at all levels should embark on aggressive health enlightenment campaign to further sustain these practices and also improve the acceptance and implementation of the practices of other child survival strategies yet to be accepted by mothers.
Keywords: Child Survival, Strategies, Assessment, Acceptance
Introduction
Child survival strategies is a concept mainly implemented in under five- clinic which is derived from the well-baby clinic of the developed world, for comprehensive healthcare for children under the age of five.1 This clinic provides preventive services along with health supervision, treatment, nutritional surveillance and health education. The important causes of morbidity and mortality of this group are mainly acute respiratory tract infection, diarrhoea, childhood anaemia, neonatal and perinatal diseases, and childhood infections. These conditions are mostly preventable with adequate healthcare and regular monitoring of growth and development.1 Child survival strategies were developed by the World Health Organisation (WHO) in collaboration with the United Nation Children Fund (UNICEF) and the World Bank as a set of evidence based intervention, which when properly implemented would reduce under-five mortality.2 Child survival strategies include; growth monitoring, oral rehydration therapy, breastfeeding and immunization, family planning, female education, food supplementation and vitamin A administration giving the acronym “GOBIFFFA”.2
Currently, child survival strategies now centred around newer strategies such as antenatal care attendance, skilled birth attendance at delivery, and commencement of breastfeeding within one hour of delivery. Others include the use of insecticide treated bed nets, management of fever, and treatment of acute respiratory infections amongst others. The child survival strategies adopted and implemented by the government of Nigeria to improve child survival and reduce morbidity/mortality of under-five children, involved interventions like maternal and new-born healthcare, appropriate treatment of major childhood diseases, vaccination against preventable diseases, nutritional intervention, malaria prevention and treatment, water and sanitation.3 Nigeria with an under-five mortality rate of 187 per 1,000 ranks fifteenth position in the world. This value is poor when compared to other countries of the world.4
Inadequate knowledge of the practices of child survival strategies by care givers as well as myths and misconceptions, contribute to child mortality and morbidity. Several factors have been linked with infant and child survival , morbidity and mortality such as maternal education, early marriage, place of residence, regional variations, short birth interval, fertility behaviour, breastfeeding practice, the use of health services by mother and child, child sex, ethnicity and religion.4 In spite of public health awareness over the last decade, sub-Saharan Africa continues to have the highest under-five mortality death in the world at 85 deaths per 1000 in 2015.5 Globally, Nigeria ranks second to India with the highest number of neonatal deaths. Nigeria demographic health survey suggests that about one in every eight children dies before their fifth birthday, approximately 21 times the average rate in developing countries.5
It is against this backdrop that the researchers deemed it fit to undertake a study of the knowledge and practices among mothers on child survival strategies in some selected Local Government Areas of Rivers State, Nigeria.
Review of Selected child survival strategies and their importance to the health of the child
Virtually all the child survival strategies have tremendous effects on improving the well-being of the child under five years of age, but the main focus in this study was on the ones below as applicable in our environment.
Skilled Birth Attendance: This strategy involves expertise care of a woman during pregnancy, labour and the provision of essential new-born care by a skilled birth attendant (SBA) to reduce neonatal mortality. However Aminu, estimated that 46 million women are likely to deliver alone or without adequate care.6 The training of lower-level and middle-level healthcare workers such as community health workers is advocated to perform specific task that may otherwise be performed by higher-level staff that takes a longer time and more expensive to train. This is effective in increasing the availability and quality of maternal and new-born care services.
Exclusive Breastfeeding: Exclusive breastfeeding has so many benefits because breast milk contains all the nutrients an infant needs for the first six months of life. WHO recommends that infants should be breastfed for the first six months of their lives to achieve optimal growth, development and health. Breastfeeding has tremendous advantages of protection against diarrhoea and many types of infections such as; respiratory tract infection, meningitis etc. Breastfeeding improves responses to vaccines by actively stimulating the immune system of children, hormones, growth factors, cytokines and even whole cells are present in breast milk and act to establish biochemical and immunological communication between mother and child.7
Growth Monitoring: Growth monitoring and Promotion (GMP) is a preventive activity comprised of growth monitoring (GM) and promotion that serves as the core activity in an integrated child health and intervention program. Growth monitoring is regular measurement of a child’s size in order to document growth. The child’s size measurement must then be plotted on a growth chart. This is extremely important as it can detect early changes in the child’s growth. Both growing too slow or too fast may indicate a nutritional or other health problem. Therefore growth monitoring is an essential part of primary health care in children.8
Immunization: According to WHO/UNICEF childhood immunization remains an important strategy in the reduction of child morbidity and mortality from common vaccine-preventable diseases which have been implicated in the death of more than 20% of children under the age of five.2
Increase in vaccine coverage has therefore been seen as an important strategy for reducing infant and child mortality rates. There has been series of coordinated global efforts to increase immunization rates in developing countries as a means of achieving improvements in child health, including the expanded program on immunization and global alliance for vaccines and immunization. For instance, the introduction of the measles vaccine in some African communities in the 1980s led to a far greater reduction in overall childhood mortality in measles alone.9
Family Planning: Family planning is the deliberate practice of controlling the timing and number of pregnancies in women. According to Freidoony et al ,intervals of at least 36 months was associated with the lowest mortality and morbidity levels at that gap for adequate provision of micronutrients before next pregnancy in women which prevents delivery of low birth weight babies.10 More so, birth defects have been common amongst children born within a year of their previous birth. Family planning helps promote child health and ensures survival as adequate attention is given to take care of the child.10
Methodology
Research Design: A descriptive survey design was used by the researcher in this Study.
Study Location: The study was carried out in some selected local government areas of Rivers state, Nigeria.
Study Population: The population of the study group comprised Residents in River State with a population of 5,198,716 (2006 census). The target population however were mothers with child/ children under the age of five years whose responsibility was to implement the child survival strategies for their children.
Sample Size: A sample size of 600 was adopted for the study.
Sampling Technique: Stratified random sampling and purposive sampling technique was adopted to select mothers of at least one child under five years old. Stratification was done based on the senatorial districts in the state. In each senatorial district, 200 respondents were randomly selected as the sample for the study.
Data collection: The researcher used a self-structured questionnaire. The questionnaire was developed in accordance with the variables and was administered with the assistance of trained nursing personnel. The questionnaire was divided into two sections. Section A elicited information on socio-demographic characteristics of the respondents while section B focused on questions showing items related to the study.
Method of Data collection: The data generated was collated and computed descriptively using frequencies and percentages. The descriptive analysis was done manually. The data analysed item by item to indicate the frequencies.
A letter of introduction endorsed by the coordinator of the school of post basic paediatric programme in the University of Port Harcourt teaching hospital was tendered to the chief nursing officers in charge of the primary health centres in the selected local government areas in each of the senatorial districts to facilitate the researchers access to the clinic for research work. The questionnaires were issued to the respondents on clinic days and were collected after being properly filled at the end of the clinic days.
Ethical Consideration: The researchers considered some ethical principles to safeguard the interest, right and safety of the respondents and strict confidentiality of the process was followed.
Results
Table 1: Socio demographic characteristics of respondents (N = 600)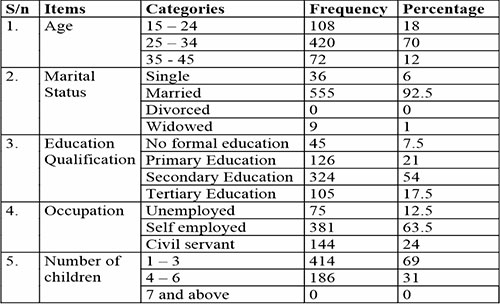
Table 1 shows socio-demographic characteristics of mothers who were selected for the assessment of child survival strategies through knowledge and practices in some local government area of Rivers state.
Table 1 shows that out of 600 respondents who took part in the study, majority were within the age of 15 – 24 years, 420 (70%) and majority were married 555 (92.5%). Also out of 600 respondents majority had primary school education, 324 (54%) while 381 (63.5%) were self-employed. Similarly, 414 (69%) of the respondents had 1 – 3 children.
Table 2: Mothers knowledge of child survival strategies (n = 600)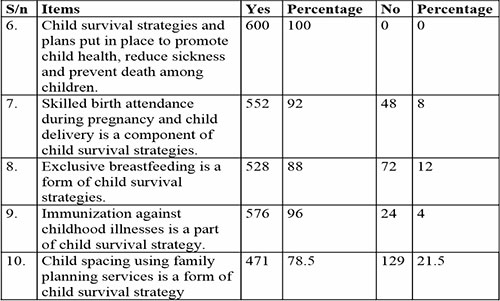
The result in table 2 shows that all respondents (100%) have good knowledge of survival strategies as plan put in place to promote child health, reduce sickness and prevent death among children. Also, 552 (92%) identified skilled birth attendant as a component of child survival strategy while 534 (88%) agreed that exclusive breastfeeding is a form of child survival strategy. Similarly, 576 (96%) identified immunization as part of child survival strategy. More so, 471 (78%) of the respondents know about family planning services as a component of child survival strategy in the study area.
Table 3: The practices of child survival strategies by mothers (n = 600)
From the above analysis provided in table 3, out of 600 respondents studied, majority 492 (82%) of the respondents were supervised by skilled child birth attendants during pregnancy and delivery conducted in a standard facility. Also 516 (86%) of the respondents actually did exclusive breast feeding for their child for complete six months. Majority 591 (98.5%) of the respondents completed all immunization for the child’s age. However, for the use of family planning services for child spacing, 504 (84%) of them were not making use of these services.
Finding of table 4 shows that out of 600 respondents studied, majority of them 516 (86%) agreed that a mother’s level of education and enlightenment is a factor that can influence the practice of child survival strategies, while for the distance and inadequate income, majority 411 (68.5%) of the respondents were of the opinion that it cannot influence the practice. In addition, 321 (53.5%) of the respondents were of the opinion that the attitude of health workers and availability of health services can influence the practice of child survival strategies.
Discussion
The findings of this study shows that a higher percentage (100%) of mothers knew that child survival strategies are plans put in place to promote healthy children, prevent sickness and death among children. However, these findings are in disagreement with the study carried out by Abimbola et al where they showed lack of knowledge11 among the women surveyed. This may have been due to their lack of information concerning the services rendered regarding the components of child survival strategies. However, the study carried out by Etokidem et al is in agreement with this study.2 It revealed that 67.3% of their respondents knew about child immunization as part of child survival strategies. The greater knowledge from the study may be due to the fact that most of these components are scheduled and delivered simultaneously during antenatal and child welfare clinics at the facilities.
Similarly, the practice of child survival strategies from the survey showed that a higher percentage of mothers (82%) actually made use of skilled birth attendants during pregnancy and delivery, while 86% of the mothers indicated that they did exclusive breastfeeding for their child for at least six months, and 95% of the mothers completed all immunization for their child’s age. Meanwhile, only 16% of the mothers made use of the family planning services in their health facilities.
The above findings are in agreement with Etokidem et al whose study showed that 62% of their respondents had the antenatal care monitored by a skilled birth attendant.2 This is in contrast to the findings of the study by Kanu et al which revealed that only 46.8% of mothers had their child birth with a skilled birth attendant and in the health facility.12 The outcome of this study is in consonance with the study by Dada where a good percentage (93.8%) practiced timely and complete immunization of their children.13 Moreover, Etokidem et al showed a 67.3% compliance with immunization.2 This study is therefore, a good outcome towards achieving the sustainable goal of health of children.
However, concerning the practice of family planning, only 16% of mothers made use of the services in the health facility. This is in contrast with resuts by Kipp et al who reported a huge coverage for contraceptives by 79% of the respondents.14 The findings above showed poor practice and use of family planning services in this study area despite a high percentage (70%) being in the peak of their reproductive years and having children ranging from three to six in number. Consequently, considering the scarce resources and economic condition in the society today, one would be right to predict a future where the children will not be properly cared for due to scarce resources and demand for child care. It therefore implies that there is a need for massive campaign and enlightenment for the mothers who are in the peak of their reproductive years to allay every fear, myth and misconceptions about family planning services to help promote the health of children and mothers.
The factors that affected the acceptance of these strategies among mothers as illicited from the questionnaire showed that a higher percentage (86%) agreed that the mother’s level of education and enlightenment, attitude of the health workers and availability of health workers can influence the practice of child survival strategies. These findings are in agreement with the study by Kanu et al whose multivariable regression analysis of 61.6% showed that education is associated with knowledge and more so significantly with improved health knowledge.12 Also from their study, absence of the care providers at the clinic at the time of health needs was identified as factors that influence the practice and utilization of child survival strategies. From the study, empowering communities especially the women with appropriate health information is a cost effective means of achieving health related goals. Similarly, Dada supported the above findings by reaffirming the importance of female education in the practice of child survival strategies, and good nutritional outcome of children emphasized as a basic knowledge of child health and nutrition should continue to be made available to women and included in school curricula.13 However in this study, a higher percentage 68.5% where of the opinion that the distance and family income cannot influence the utilization of child survival strategies. This is in contrast with Kanu et al who described distance to health facility (63.5%) and lack of income (87.3%) as some of the indices that can affect the utilization of health services of child survival strategies.12 The mothers were of the opinion that distance cannot stop any mother as she can trek miles to do the right thing concerning the health and life of the child. This is a new trend where mothers are willing to go the extra miles for the wellbeing of their children.
However, the implementation of child survival strategies amongst mothers had some challenges as there were lots of factors that influenced the utilization of these strategies among mothers such as; accessibility to health services, maternal literacy, level of knowledge, family socioeconomic factors and practices that show non commitment to child care by care giver.
In summary, the study has revealed that mothers from these local government areas had good knowledge of child survival strategies and its components. They also consented to the fact that they made use of these strategies available in their health facilities such as skilled birth attendance, child immunization while consistently practicing exclusive breastfeeding for their babies. However, these mothers who are in the peak of their reproductive years are yet to embrace the family planning services available in facilities despite knowing it can help in child spacing. This calls for aggressive health education and awareness creation, community mobilization to improve the level of acceptance of family planning and other child survival strategies in the community.
Conclusion
It is imperative that health personnel should be encouraged to use persuasive communication skills in their health education to convince mothers during antenatal care, child welfare clinics, home visits on survival strategies in order to improve the health of the Nigerian child, reduced morbidity and mortality while ensuring happy family and home.
References
- Datta SS, Rangaratham P, Sivakumar KS. A study to access text messaging service in delivering maternal and child health care messages in a rural area of Tamil Nadu, India. Austalian Medical Journal.2014;7(4):175-80
- Etokidem AJ, Johnson O. Child survival strategies: Assesment of knowledge and practice of rural women of reproductive age in Cross River state, Nigeria. Journal of tropical Medicine.2016; 8.1-6
- WHO/UNICEF World health Organisation/United Nation Children Fund Regional child survival strategies; Acelerated and sustained action towards MDG 4.2015
- Okoh BAN, Alex-Hart BA. Home management of diarrhoea by caregivers presenting at diarrhoea training unit of a tertiary hospital in Southern Nigeria. British Journal Of Medicine & Medical Research.2014, 4(35) ;5524 - 5540.
- Morakinyo OM, Fagbamigbe AF. Neonatal, infant and under-five mortalities in Nigeria. An examination of trends and drivers (2003-2013). PLOS ONE 2017;12(8):e0182990.
- Aminu M. Reducing neonatal mortality through skilled birth attendant.Human resources for health. The lancet globalhealth blog. 2004. Retrieved from global health.
- Labiok MH. Effects of breast feeding on the mother. Paediatric clinic of North America, 2001; 48 (1) 143 - 158.
- Feleke FW, Adole AA, Afework MB. Utilization of growth monitoring and promotion services and associated factors among under two years of age children in southern Ethopia; pLos one 2017, 12(5):e0177502.
- McGovern ME, Canning D. Vaccination and All-cause Chid mortality from 1985 to 2011. Global Evidence from Demographic and health Surveys, American Journal of Epidemioogy. 2015, 182: (9) 791-798.
- Freidoony L, Ranabhat CL, Kim CB, Kim CS, Ahn D, Doh YA. Predisposing, enabling and need factors associated with utilization of institutional delivery services: A community-based cross-sectional study in far-western Nepal, Women & Health.2018, 58: (1) 51.
- Adebowale Y, Fagbamigbe AF. Survival probability and predictors for woman experience childhood death in Nigeria, analysis of North - South differentials. BMC Public Health 2012, 12:430
- Kanu JS, Tang Y, Liu Y. Assessment of the knowledge and reported practises of women on maternal and child health in rural Sierra Leone. A cross sectional Survey PLOS ONE 2012;9(8):e1059
- Dada P. A survey of child survival strategies in Ishiala Ngwa south L.G.A, Abia state, Department of environmental health technology, college of health technology. 2011.
- Kipp AM, Mambolwa M, Brault MA, Kalesha M, Katepa-Bwalya M, Habimana P. Improving access to child health services at the community level in Zambia. A Country case study on progress in child survival (2000-2013). Health policy and planning 2017;32:(5) 603-612.