A study on Awareness and Knowledge of Surgical Site Infection among Dental Patients in a Nigerian Tertiary Hospital
Igbinosa L1, Edetanlen EB2, Babalola O3
Abstract
Background: Risk of surgical site infection (SSI) can be reduced or eliminated if its awareness and knowledge is optimal among patients.
Aim: The aim of this study was to assess the level of awareness and knowledge of SSI among dental patients in a Nigerian Tertiary Hospital.
Materials and methods: This was a cross-sectional study design conducted in hospital setting on adult Nigerian population visiting a tertiary hospital between December, 2022 and February, 2023. The data was collected with a pretested 36-item, structured, close-ended, self-administered and interviewer -administered questionnaires. The data collected were socio demographic characteristics, past admission, days of hospitalization, reason for admission and history of SSI. Other collected data were awareness and knowledge of SSI. Both descriptive and inferential statistics were analyzed. The data was entered and analyzed using the statistical package for the social sciences (SPSS), version 26 (IBM, Armonk, NY, United States of America). A critical probability level (p-value) of <0.05 was used as the cut-off level for statistical significance.
Results: A total of 102 dental patients were interviewed in this study. The age range and the mean age were 20 -76 years and 45.3± 5.1 years respectively. There was slight (55.9%) preponderance of female gender. Only 24(23.5%) respondents had heard of SSI and this was mainly through medical personnel. The majority (76.5%) of the respondents had never seen anyone diagnosed of SSI. Few (6.9%) respondents claimed they were enlightened about SSI prior to surgery. Overall, half (50%) of the respondent had poor knowledge while only 13(12.7%) had good knowledge. Marital status, level of education and previous admission were significantly associated with poor knowledge (p<0.05).
Conclusions: The awareness and knowledge of surgical site infection among patients in this study were relatively poor. Therefore, awareness campaign among Nigerian population can help improved the level of knowledge for better wound care and quality care.
Key words: Awareness, knowledge, Surgical Site Infection, Dental Patients, Nigerian Tertiary Hospital.
Introduction
Though several definition of surgical site infection (SSI) exist in the literature, the most widely used and accepted definition is the 1992 reclassification and definition by United States of America Centre for Disease Control and Prevention (CDC) which defined SSI as “an infection that occurs after surgery in the part of the body where the surgery took place within 30 days of an operative procedure or within one year if an implant is left in place.”1 It affects either the incision or deep tissue at the operation site and may require surgical intervention.2
Globally, the rates of SSI remain considerably high despite advances in surgical techniques and this cut across all surgical procedure such as oral and maxillofacial surgeries, general surgeries, appendectomies.3-5 SSI rates differ across countries depending on various factors.3,6,7 In Nigeria, SSIs have been reported to be 45.8%, 16.2%, and 16.7% following orthopaedic surgeries, appendectomies and obstetrics and gynecological surgeries respectively.8-10 SSI is a considerable disease and healthcare burden, as it increases hospitalizations, costs, and mortality rates.11 In developed countries, SSI increases the average hospital length of stay that can result in an annual additional cost.2 In developing countries, SSI can pose a serious economic burden.12 Therefore, there is need to lower the rates of SSIs worldwide. One of the effective strategies for SSI prevention is increasing patient engagement.13 Studies14-18 have reported a gap in patient engagement to reduce SSIs. To develop effective engagement strategies, it is important to understand the current knowledge and awareness of SSI among patients.
Though retinues of studies19-24 were found in the literature on awareness and knowledge of SSI among health care providers, it appears few studies25,26 were reported only in the developed countries. To the best of our knowledge, none was found among dental patients. Therefore, the aim of this study was to evaluate the awareness and knowledge of SSI among dental patients in a Nigerian teaching hospital. The findings of this study would aid in the development of SSI preventative strategies in Nigeria.
Materials and method
Ethical consideration: Prior to commencement of the study ethical approval was not sought from the Research and Ethics Committee of the University of Benin Teaching Hospital.
Study setting: This study conducted between December, 2022 and February, 2023 at dental complex of a Nigerian teaching hospital. This hospital serves as one of the main government healthcare centers in southern Nigeria and have a high volume of surgical procedures.
Study design: This was a cross-sectional study design.
Sample size calculation: The minimum sample size of 96 was determined using the statistical formula of Cochrane27 for sample size calculation: N= Z2P (1-P)/ d2. Where N is the minimum sample size for a statistically significant survey, Z is normal deviant at the portion of 95% Confidence Interval (C.I) = 1.96, Since this is preliminary study in Nigeria, a best guess prevalence of 50% was chosen for the estimation of sample size,28 and d is margin of error acceptable or measure of precision = 10%. However, the sample size was increased to 102 to compensate for non-responses.
Study population: The study population was all adult Nigerians. All participants were provided with relevant information regarding the study and informed consent was obtained from them. The participants’ responses were held in strict confidence. There were no identifiers on the questionnaire to maintain anonymity. Access to questionnaires was restricted. The study did not pose any risk or harm to the research participants. Recruitment was based on participants’ voluntariness to take part in the study. They were free to withdraw their consent at any time.
Inclusion and exclusion criteria: Included in the study were any adult Nigerian who gave their consent to be included in this study and who came to our facility for treatment; able to understand, read, speak or write English; and capable of answering the questions either in written form or by interview. The questionnaire was self-administered and interviewer administered. Excluded were those that did not give consent to participate in the study.
Sampling method: All eligible samples was recruited based on non‑randomized convenience sampling technique.
Study instrument: The tool used in this study was validated in a previous study.26 The data was collected with 36-item, structured, close-ended, self-administered questionnaire which was pretested for feasibility. The questionnaire was in English and categorized into four sections. The first section of seven items elicited the demographic information (age, gender, marital status, level of education, occupation, religion and ethnicity). The second section of 4 items investigated the clinical characteristics such as previous admission reason for admission, day of admission and history of SSI. The third section with 7 questions was on the awareness of SSI and the last section with 8 questions was on knowledge of SSI. To determine the level of knowledge, any positive response was scored 1 while negative response was scored 0 and the overall score was 0-8. Score from 0-2 was considered as poor, 3-5 as fair and 6-8 as good. The questionnaire was pilot tested in 10 randomly chosen samples following which no additional changes were deemed necessary; these responses were not included in the full‑scale study analyses. The reliability of the questionnaire was assessed using Cronbach’s alpha and was found to be 0.8.
Data management: The data collected were age, gender, department of respondents, medical status, years of experience, additional degree. Other collected data were awareness, knowledge, and practice of radiation protection. Both descriptive and inferential statistics were analysed. In the descriptive statistics, the categorical variables were expressed in frequency and percentages while numerical variables were expressed in mean and standard deviation. In the inferential statistics, Chi-square test was used to found any association between the dependent and independent variables. The data was entered and analyzed using the statistical package for the social sciences (SPSS), version 26 (IBM, Armonk, NY, United States of America). A critical probability level (p-value) of <0.05 was used as the cut-off level for statistical significance.
Results
Table 1: The sociodemographic characteristics of the respondents (n=102)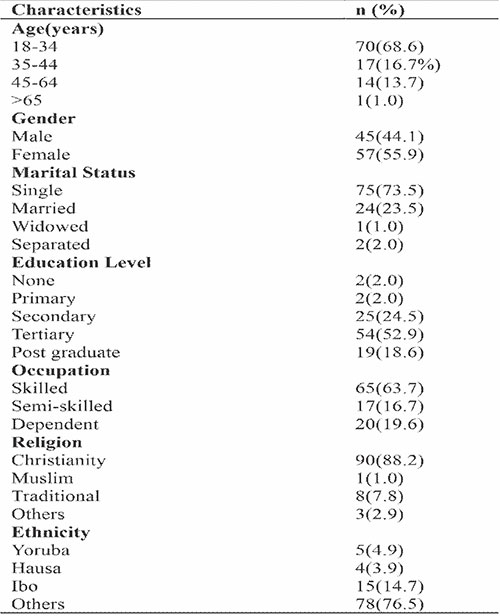
Table 2: The clinical characteristics of the respondents (n=102)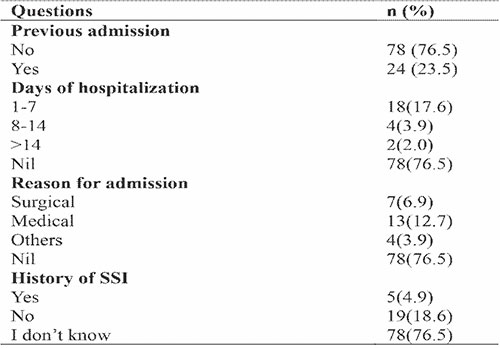
Table 3: The level of awareness of SSI among the respondents (n=102)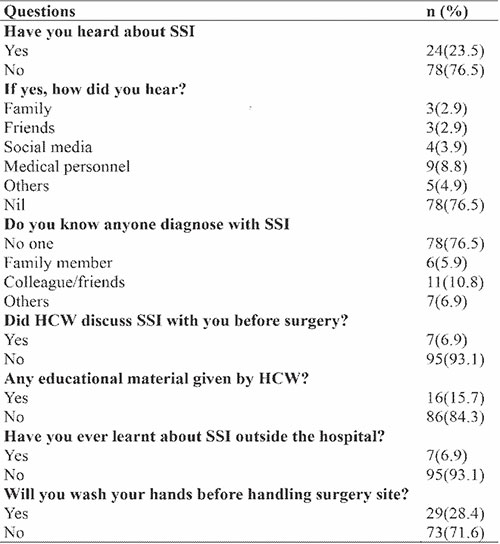
Table 4: The level of knowledge of SSI by the respondents (n=102)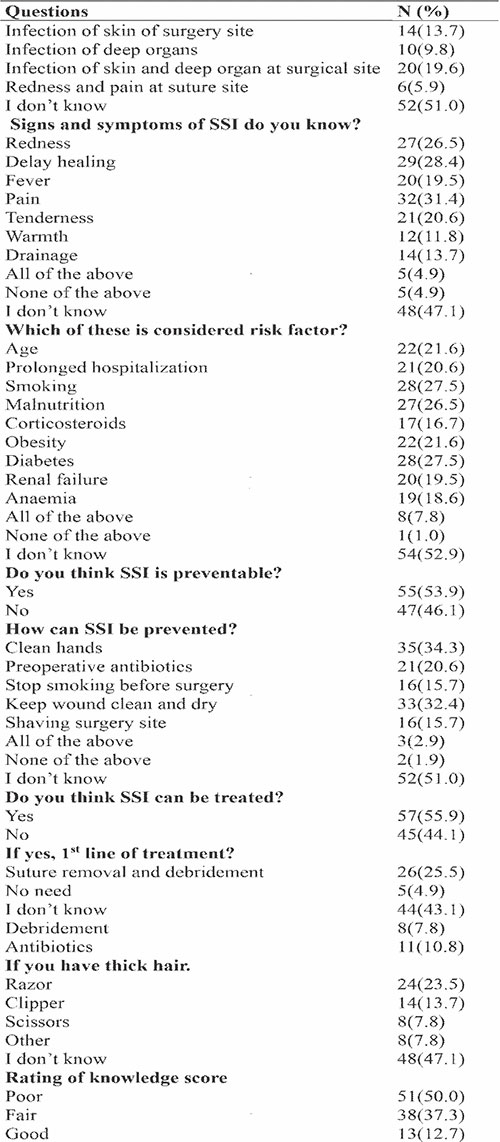
Table 5: The effect of sociodemographic characteristics on poor knowledge of SSI among the Nigerian population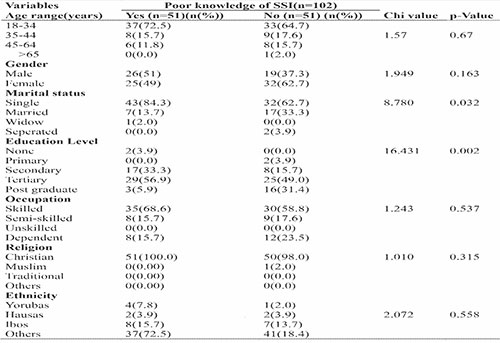
Table 6: The effect clinical characteristic on poor knowledge of SSI among the Nigerian population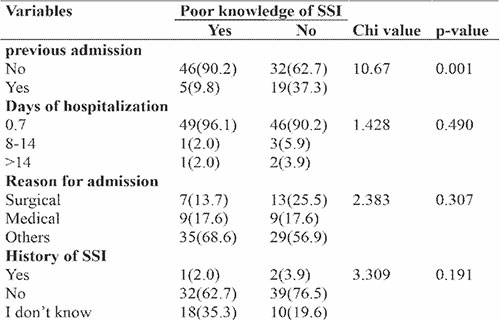
A total of 102 dental patients were included in this study. The age range and the mean age were 18-76 years and 45.3 ± 5.1 years respectively. Table 1 shows the demographic characteristics of the respondents.
Most (68.6%) of the respondents were within the age range of 18-34 years while the least (1%) were those older than 65 years. There was slight (55.9%) preponderance of female gender. Two-third (73.5%) of the respondents was singles. Slightly more than half (52.9%) of the Nigerian population recruited had a tertiary level of education and more than half (63.7%) of the respondents were skilled workers. Majority of the respondents were Christians. Most (76.5%) of the respondents were not of the major ethnic groups in Nigeria and this was followed (14.7%) by the Ibos.
Table 2 shows the clinical characteristics of the respondents. Of the total number of respondents, almost two-third (76.5%) had no previous admission history and for the that were previously admitted, only 2(2.0%) had hospital stay greater than 14 days the admission was mainly (12.7%) due to medical conditions. For those that were admitted due to surgical reasons, only 5 had a history of SSIs.
Table 3 shows the level of awareness of SSI among the respondents. Just only 24(23.5%) respondents had heard of SSI and this was mainly through medical personnel. The majority (76.5%) of the respondents had never seen anyone diagnosed of SSI. Just few (6.9%) respondents claimed they were enlightened about SSI prior to surgery. Surprisingly, majority (71.6%) of the respondents are not aware of hand washing before touching surgical wounds.
Table 4 shows the level of knowledge of SSI by the respondents. More than half (51%) of the respondents do not know what is SSI. Greater (47.1%) number of the respondents could not identify any signs and symptoms of SSI. In the same va in, more than half (52.9%) of the respondents could not identify any risk factor of SSI. Though more than half (53.9%) knew it is preventable but more than half (51%) do not know the preventive measures. Those that know that SSI treatable was more (55.9%) than those who don’t know but they mainly (43.1%) don’t know about the treatment. Most (47.1%) of the respondents don’t know that electric clipper is the recommended method to shave the operation site. Overall, half (50%) of the respondent had poor knowledge while only 13(12.7%) had good knowledge. Marital status and level of education were significantly associated with poor knowledge (Table 5).
History of previous admission significantly affected the rate of poor knowledge among the respondents as observed in Table 6.
Discussion
The awareness and knowledge of surgical site infection among patients visiting the dental center in a Nigerian tertiary hospital was studied. In the literature, much attention has been given to the health care providers on their level of knowledge of prevention of SSI globally19-24 with little attention on the patients who their engagement can help reduce this global health burden. Though few studies are available in the developed countries25,26 however, to the best of our knowledge this is the first study to evaluate the level of awareness and knowledge of SSI among the populace in a developing country. This study is timely due to the higher rate of SSI in developing countries despite the reported adequate level of practice of prevention of SSI among the health care providers in Nigeria.8-10
The result of this study demonstrated that the prevalence of the Nigerian population that had poor knowledge was 50% and this value is alarmingly high and this is a clarion call for establishment of awareness programmes among the populace. The 50% prevalence rate in this study is higher than the 35.2% reported in a multi-centre study in Saudi Arabia in 2022 by Alsahli et al.26 The difference in prevalence could be related to variation in sample size of the recruited populations. In this study, we found difference in level of knowledge based on marital status. Being unmarried was a significant factor associated with poor knowledge of SSI. This finding is in contrast with that of a previous study25 that didn’t observe an association between poor knowledge of SSI and marital status. The difference could be to the fact that most (62.4%) respondents were married in the previous study while most (73.4%) where single in the present study. Like the study of Alsahli et al26 and Anderson et al.25 level of education was related to the level of knowledge of SSI among the population studied. This could be the fact that those with higher level of education seek information more compared to those with basic educational levels.
A total of 102 patients were interviewed in this study. To the best of our knowledge only two studies were seen in the course of literature searched that focus on patients rather than health care workers as regard SSI awareness and knowledge. Though the current study has a sample size less than the 219 recruited by Alsahli et al26 in Saudi Arabia but is higher than 52 recruited by Anderson et al25 in US. It is therefore, suggested the findings of the present study can be generalized to the Nigerian population as a whole. In this study there more female respondents and this finding is different from that reported in a previous study.26 The likely reason for this variation could be the fact that women seek health care than their opposite folks. Unlike in a previous study that reported more respondents at a secondary level of education, the current study25 found more than half of the Nigerian population that had a tertiary level of education. This implies the elites utilize health care services than those with lower level of education in developing countries like Nigeria.9 History of previous admission was found to be associated with the level of knowledge of SSI in the present study. This is in contrast with the findings of Alsahli et al26 who did not found any difference in knowledge of SSI as regard previous admission. Sample size variation could be attributable to the difference in findings.
This study had few limitations. First, it was a single centre study; however, the response rate was high. Second, the sample size could have been more though it was statistically estimated. Lastly, being the first to evaluate awareness and knowledge of SSI among non-health caregiver in my clime, it comparison of its findings was challenging.
Conclusion
The awareness and knowledge of surgical site infection among dental patients in a Nigerian population were relatively poor. Therefore, awareness campaign among Nigerian population can help improved the level of knowledge for better wound care and quality care.
Acknowledgement: We want to thank other consultants in our health facility for allowing us to recruit their patients in this study. Our appreciation also goes to the board of management for the opportunity to perform this study.
Conflict of interest: There are no conflicts of interest
Funding: Nil
References
- Centre for Disease Control. Surgical Site Infection (SSI) Event. Procedure-Associated Module SSI; Centre for Disease Control: Atlanta, GA, USA, 2017. Available online: www.cdc.gov (accessed on 21 July 2017).
- Yousef AL‑Aali K. Evaluation of surveillance for surgical site infections and drug susceptibility patterns, Taif, Saudi Arabia. Ann Clin Lab Res 2016;4:2
- Danwang C, Mazou TN, Tochie JN, Nzalie RN, Bigna JJ. Global prevalence and incidence of surgical site infections after appendectomy: A systematic review and meta‑analysis protocol. BMJ Open 2018;8:e020101.
- Gillespie BM, Harbeck E, Rattray M, Liang R, Walker R, Latimer S, et al. Worldwide incidence of surgical site infections in general surgical patients: A systematic review and meta‑analysis of 488,594 patients. Int J Surg 2021;95:106136.
- Danwang C, Bigna JJ, Tochie JN, Mbonda A, Mbanga CM, Nzalie RN, et al. Global incidence of surgical site infection after appendectomy: A systematic review and meta‑analysis. BMJ Open 2020;10:e034266.
- Fan Y, Wei Z, Wang W, Tan L, Jiang H, Tian L, et al. The incidence and distribution of surgical site infection in mainland China: A meta‑analysis of 84 prospective observational studies. Sci Rep 2014;4:6783.
- Al‑Kenani N, Alsultan A, Bahkali M, Alosfoor M, Al‑Mohrej O. Incidence and predictors of surgical site infections following foot and ankle surgery. J Musculoskelet Surg Res 2017:1:1;6‑9.
- Olowo-Okere A, Ibrahim YKE, Sani AS, Atata RF, Olayinka BO. Prevalence of Surgical Site Infection in a Nigerian University Teaching Hospital. J. Pharm. Allied Sci. 2017, 14, 2430–2438.
- Atata RF, Ibrahim YKE, Olurinola PF, Adigun IA, Giwa A, Ii A. Prevalence of Surgical Site Nosocomial Infection in A Tertiary Health Care Institution in Nigeria. Int. J. Epidemiol. Infect. 2013; 1:52–57.
- Adejumo AA, Nuhu M, Afolaranmi T. Incidence of and risk factors for abdominal surgical site infection in a Nigerian tertiary care centre. Int. J. Infect. Control 2015, 11, 1–12.
- Jenks PJ, Laurent M, Mcquarry S, Watkins R. Clinical and economic burden of surgical site infection (SSI) and predicted financial consequences of elimination of SSI from an English hospital. J. Hosp. Infect. 2014, 86, 24–33.
- Birhanu Y, Endalamaw A. Surgical site infection and pathogens in Ethiopia: A systematic review and meta‑analysis. Patient Saf Surg 2020;14:7.
- Mbamalu O, Bonaconsa C, Nampoothiri V, Surendran S, Veepanattu P, Singh S, et al. Patient understanding of and participation in infection‑related care across surgical pathways: A scoping review. Int J Infect Dis 2021;110:123‑34.
- Ardizzone LL, Smolowitz J, Kline N, Thom B, Larson EL. Patient hand hygiene practices in surgical patients. Am J Infect Control 2013;41(6):487–91.
- Berger Z, Flickinger TE, Pfoh E, Martinez KA, Dy SM. Promoting engagement by patients and families to reduce adverse events in acute care settings: a systematic review. BMJ Qual Saf 2014;23(7):548–55.
- Levinson W, Kao A, Kuby A, Thisted RA. Not all patients want to participate in decision making. J Gen Intern Med 2005;20(6):531–5.
- Longtin Y, Sax H, Leape LL, Sheridan SE, Donaldson L, Pittet D. Patient participation: current knowledge and applicability to patient safety. Mayo Clin Proc 2010;85(1):53–62.
- Muir R, Carlini JJ, Harbeck EL, Gillespie BM, Tuffaha HW, Walker RM, et al. Patient involvement in surgical wound care research: a scoping review. Int Wound J 2020;17(5):1462–82.
- Kolade OA, Abubakar S, Adejumoke SR, Funmilayo HV, Tijani A. Knowledge, attitude and practice of surgical site infection prevention among post-operative nurses in a tertiary health institution in north-central Nigeria. International Journal of Nursing and Midwifery 2017; 9(6): 65-69.
- Sadaf S, Inayat S, Afzal M, Hussain M. Nurse’s knowledge and practice regarding prevention of surgical site infection at allied hospital Faisalabad. International Journal of Scientific and Engineering Research 2018; 9(5): 351-369.
- Yang Y, Cheng J. Survey of operating room nurses’ knowledge and practice on surgical site infection prevention. Chinese Journal of Nurses Training, 2014; 29(20):1894-1896.
- Bhangu A, Ademuyiwa AO, Aguilera ML, Alexander P, Al-Saqqa SW, Borda-Luque G, et al. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: A prospective, international, multicentre cohort study. The Lancet Infectious Diseases 2018;18(5): 516-525
- Zhou F, Huang Q, Lei X. Medical staffs’ knowledge, attitude, and practice on surgical site infection prevention in primary hospitals. Chinese Journal of Today Nurse 2014; 10: 122-124
- Woldegioris T, Bantie G, Getachew H. Nurses' Knowledge and Practice Regarding Prevention of Surgical Site Infection in Bahir Dar, Northwest Ethiopia. Surg Infect. 2019;20(1):71-7.
- Anderson M, Ottum A, Zerbel S, Sethi A, Gaines ME, Safdar N. A survey to examine patient awareness, knowledge, and perceptions regarding the risks and consequences of surgical site infections. Am J Infect Control 2013;41:1293‑5.
- Alsahli AM, Alqarzaie AA, Alasmari AM, AlOtaibi MM, Aljuraisi AM, Khojah AA, et al. Awareness and knowledge of postoperative surgical site infections in patients from Saudi Arabia: A multi‑regional cross‑sectional study. Saudi J Med Med Sci 2022;10:243-52.
- Cochrane WG. Sampling Techniques, 3rd ed. New York: John Wiley and Sons.1977
- Araoye MA. Research methodology with statistics for health and social sciences. 1st ed. Illorin: Nathadex . 2003; 35: 115-121.