Predictors of expressed emotion among the caregivers of patients with severe mental illnesses attending a tertiary health facility in Kano
Aghukwa NC1, Baguda AS1, Fawaz B2, Aminu IS1
Abstract
Background: Expressed Emotion (EE) measures the emotional climate between caregivers and patients with major mental disorders. High EE could trigger relapses in schizophrenia and other conditions. However, the factors influencing high EE were poorly understood, especially in Africa. This study explored the socio-demographic, personality, and patient-related predictors of high EE among caregivers in Kano.
Objectives: The study aimed to estimate the prevalence of high EE and its associations with socio-demographic factors, personality traits, and patients’ illness characteristics.
Methods: The study utilized a descriptive cross-sectional design, encompassing 270 patients diagnosed with schizophrenia or bipolar disorder, each accompanied by their corresponding caregiver, totalling 270 caregivers. All participants attended the psychiatric clinic at Aminu Kano Teaching Hospital. The data collection process involved questionnaires and interviews, addressing socio-demographics, illness characteristics, personality traits, and expressed emotion (EE).
Results: We analyzed the socio-demographic factors and EE of 250 patients and their corresponding 250 caregivers. High EE was prevalent (42.8%) due to critical comments and emotional over-involvement. Caregivers scored high on all personality traits, but only neuroticism correlated positively with EE (r = 0.130, p < 0.05). EE was lower for bipolar disorder than for schizophrenia (r = -.126, p < .05). EE also increased with patient symptoms, caregiver burden, and relapse frequency.
Conclusion: Caregivers of patients with schizophrenia and bipolar disorder in Kano showed high expressed emotion (EE). However, none of the analyzed factors, including socio-demographic and personality traits, emerged as significant predictors of EE. Further research is needed to improve interventions and support strategies for caregivers of individuals with severe mental illnesses.
Keywords: Expressed Emotion, Caregivers, Mental Illness, Predictors
Introduction
Expressed Emotion (EE) is a pivotal measure in understanding the intricate dynamics between caregivers and individuals grappling with major psychiatric disorders. Although the association between high EE and relapse risk in schizophrenia and other mental conditions is well-established, the factors influencing high EE, particularly in Africa, remain inadequately explored.1,2 This research aims to bridge this gap by investigating these factors among caregivers of individuals with major mental disorders in Kano, Nigeria.
The roots of Expressed Emotion trace back to the late 1950s and 1960s in the United Kingdom, marked by seminal studies identifying abnormal caregiver interactions and attitudes.3,4 Components of EE, including criticism, hostility, emotional over-involvement, warmth, and positive regard, have undergone assessment through various tools, evolving from the Camberwell family interview to the 5-minute speech sample and the Family Questionnaire interview.4-7 Beyond schizophrenia, global research indicates the universal nature of EE, extending its association with relapse risk to diverse mental disorders such as dementia, autism, and eating disorders.8-10
Prevalence studies on expressed emotion (EE) among caregivers of individuals with major mental disorders primarily focus on high EE. However, regional variations persist. For example, caregiver prevalence of high EE among people with schizophrenia ranges from 12% in Bali to 80.65% in southern Nigeria.11,12 The relationship between socio-demographic characteristics and EE yields mixed findings, with some studies suggesting associations between factors like education and economic status.13-15 However, exploration of the relationship between caregiver personality traits and EE remains limited.16-18
Critical comments are part of the negative components of EE, implying that caregivers who are highly critical of a patient are more likely to be high EE caregivers. Some researchers have established that being a highly critical caregiver is dependent on the personality of the caregiver, to the extent that the personality trait of a caregiver plays a role in the genesis of critical comments more than the severity of the patient’s illness.1,19 In another study, it was established that patients who display high EE attitudes were likely to be unsatisfied with their lives, pessimistic about their future, and tended to show reduced self-efficiency. The authors added that high EE caregivers scored less on flexibility, tolerance, and empathy when compared with low EE caregivers. Controllability attribution has also been used to study and explain the relationship between personality traits and EE among caregivers of patients with mental disorders. Critical caregivers have been said to be high scorers on the attribution scale, in the sense that they are more likely to believe that the patient’s symptoms are under their (the patient’s) own control.19-21
The gendered nature of caregiving responsibilities in Nigeria is the focus of Adeyemi’s thesis, which reveals that most caregivers are women, in line with global trends. The thesis also sheds light on the diverse roles of caregivers and the impact of financial burden on family activities and interactions.22 Another study by Baby Shalini et al. examines the relationship between the level of Expressed Emotion (EE) and the type of illness among caregivers of patients with major mental disorders. The study finds a significant inverse relationship between EE and the type of illness, emphasizing the intricate and context-dependent nature of these relationships.10
Building on these studies, researchers from Bayero University and Aminu Kano Teaching Hospital explore the relationship between caregiver EE, quality of life (QoL), and medication adherence in individuals with schizophrenia in Nigeria.23 Their findings indicate that high caregiver EE is associated with lower QoL and, to some extent, poor medication adherence among patients with schizophrenia. Conversely, medication adherence positively correlates with higher overall, health-related, and physical domain QoL.23 This study not only enriches the broader understanding of the intricate dynamics between caregivers and individuals grappling with major psychiatric disorders but also serves as a relevant precursor to our investigation. The significance of our research extends beyond academic realms, with implications for healthcare education, mental health policies, and future research endeavours in the region.
The Family Questionnaire (FQ) emerges as a reliable tool for evaluating EE in families impacted by schizophrenia, providing a methodological foundation for our research. Insights from studies in the UK and among South Asian heritage families enrich our understanding of how cultural factors influence EE. However, a critical analysis reveals the need for more research considering cultural diversity and specific caregiving contexts.24,25
The Revised NEO Personality Inventory (NEO-PI-R) is a widely used measure of personality traits based on the five-factor model (FFM). The NEO-PI-R measures six specific traits that define each of the five factors: Neuroticism (N), Extraversion (E), Openness to Experience (O), Agreeableness (A), and Conscientiousness © 1. The NEO-PI-R has been validated in various cultural settings and has been used in research and clinical practice to assess personality traits and their implications for mental health. The NEO-PI-R has also been used to study the cultural and gender differences in personality traits, and the implications for the assessment and interpretation of the NEO-PI-R 1.26
This literature review offers valuable insights for our study on caregivers' EE in patients with schizophrenia and bipolar disorders at Aminu Kano Teaching Hospital. Our objectives include exploring the prevalence of high EE, investigating relationships with socio-demographic characteristics and personality traits, and understanding the impact of patients' illness characteristics on caregiver EE.
Additionally, this synthesis underscores the global nature of EE research and highlights the importance of contextualizing findings in diverse cultural settings. While the existing literature provides a solid foundation, our study in Kano, Nigeria, is poised to contribute new insights, particularly in the African context where mental health services are limited and stigmatized. The significance of our research extends beyond academic realms, with implications for healthcare education, mental health policies, and future research endeavours in the region.
The significance of our research extends beyond academic realms, with implications for healthcare education, mental health policies, and future research endeavours in the region.
Methods
Study design and setting: We conducted a cross-sectional study at the Adult Psychiatric Clinic of Aminu Kano Teaching Hospital (AKTH), a federal tertiary health facility located in Kano, northern Nigeria. The clinic, serving as a tertiary centre for patients from Kano and neighbouring states, provided an ideal setting for investigating the dynamics of expressed emotion (EE) in the context of severe mental illnesses.
Participants: Our study centered on adults diagnosed with severe mental illnesses (SMIs), specifically focusing on individuals with schizophrenia or bipolar affective disorder and their caregivers. Notably, the study ensured one caregiver per patient, emphasizing the primary caregiver's role. The inclusion criteria mandated that patients be at least 16 years old, possess a confirmed diagnosis, maintain remission status, and share living arrangements with a caregiver for a minimum of 3 months. Eligible patients were selected through systematic random sampling from the clinic register. Caregivers, who were required to be at least 18 years old, serve as the primary caregiver, and cohabit with the patient for at least 3 months, were also included in the study
Sample size: The minimum sample size was calculated using the formula for cross-sectional studies, considering a confidence level of 95%, a margin of error of 5%, and an estimated prevalence of high EE in Nigeria obtained from a previous study by Babandi et al.23 Factoring in a 10% dropout rate, the final sample size (N) was determined to be 270 patients, each accompanied by their corresponding caregiver, resulting in a total of 270 caregivers. The inclusion of both patients and their corresponding caregivers was integral to the study design.
Ethical Considerations: Ethical clearance was obtained from the Ethical Committee of AKTH, and informed consent was secured from all participants. Stringent measures were implemented to ensure confidentiality and anonymity, including assigning codes to protect participant identities. Data were securely stored, with restricted access limited to the research team.
Instruments: Data collection instruments comprised 1. Socio-demographic and Illness Questionnaires designed to gather information on patients' and caregivers' socio-demographic characteristics and illness details, 2. Big Five Inventory-2 Short Form (BFI-2-S): A 30-item self-report questionnaire assessing personality traits—conscientiousness, agreeableness, neuroticism, openness, and extraversion—for both patients and caregivers, and 3. Family Questionnaire (FQ): A 20-item self-report scale measuring the level of expressed emotion (EE) in family relationships. FQ gauged the frequency of EE, focusing on criticism and emotional over-involvement (EOI).
Data Analysis: The data were analyzed using SPSS, employing univariate and bivariate analyses. Continuous variables were presented using measures of dispersion and central tendency, while categorical variables were expressed as percentages. Multiple logistic regression was employed to identify predictors of expressed emotion among caregiver respondents. This comprehensive analysis aimed to unravel the intricate relationships between various variables and shed light on the determinants of EE in the studied population.
Results
The study meticulously explored socio-demographic aspects of patients with Schizophrenia and Bipolar Disorder, along with the expressed emotions of their caregivers. Initially targeting a sample size of 270, the study achieved a commendable 92.6% response rate, with 250 patient-caregiver pairs completing the research.
Patient demographics revealed a concentration in the 16-30 and 31-45 age brackets, a slight male predominance, and most married individuals from the Hausa ethnic group. Among caregivers, a diverse age distribution was observed, predominantly female, from the Hausa ethnic group, and practising Islam. These insights set the foundation for the subsequent sections.
Section 1: Socio-Demographic Characteristics
Tables 1a and 1b provide a comprehensive overview of the Socioeconomic and Demographic Characteristics of Patients diagnosed with Schizophrenia and Bipolar Disorder, along with their caregivers assessed for Expressed Emotions at AKTH.
Table 1a: Socioeconomic and Demographic Characteristics of Patients Whose Caregivers are Assessed for Expressed Emotions: Aminu Kano Teaching Hospital (AKTH)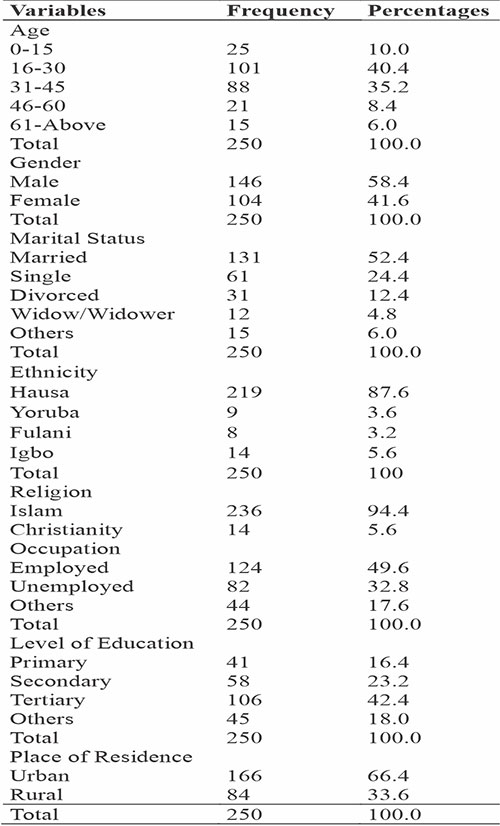
Section 2: Correlational Analysis with Socio-Demographic Characteristics
Table 1b: Socioeconomic and Demographic Characteristics of Caregivers of Patients with Schizophrenia and Bipolar Disorder Assessed for Expressed Emotions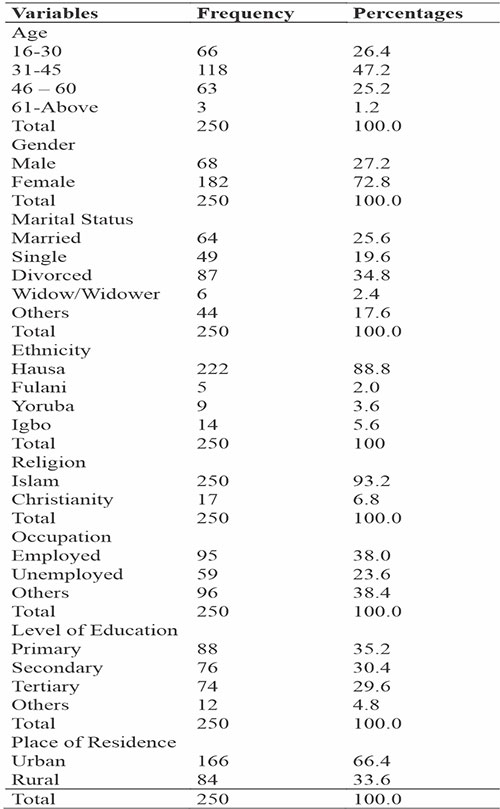
Chi-Square tests revealed no significant associations between patients’ socio-demographic characteristics and caregivers’ expressed emotions at Aminu Kano Teaching Hospital (AKTH) (p > .05) (Table 2). Symmetric Measures (Phi and Cramer’s V) indicated weak associations between patients’ demographics and caregivers’ expressed emotions at AKTH (0.01 to 0.07) (Table 2).
Table 2: Chi-square tests of association between patients’ socio-demographic characteristics and caregivers’ expressed emotions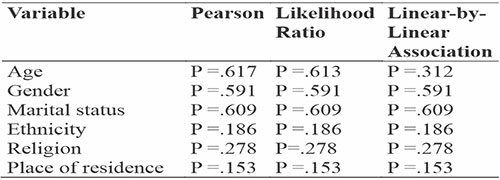
Table 3: Correlation Between Caregivers' Sociodemographic and Expressed Emotions at AKTH
Regarding gender and expressed emotion, Table 3 showed a weak, statistically insignificant negative correlation of -0.038 (p = 0.547). This implies that the observed relationship between gender and expressed emotion is likely due to chance, suggesting gender is not a significant factor influencing expressed emotion.
Table 4: Correlations Among Level of Expressed Emotion, Caregiver's Level of Education, Occupation, Religion, and Ethnicity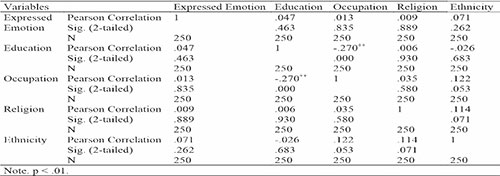
Table 4 displayed correlations between expressed emotion and caregiver characteristics. A weak positive correlation with ethnicity lacked statistical significance (r = .071, p = .262). No significant correlations were found for education (r = .047, p = .463), occupation (r = .013, p = .835), or religion (r = .009, p = .889). However, a moderate negative correlation (r = -.270, p < .01) between education and occupation suggested that higher education levels were associated with lower occupational levels among caregivers.
Table 5: A Binary Logistic Regression Analysis of Caregiver's Level of Expressed Emotion on Patients’ Socio-demographic Characteristics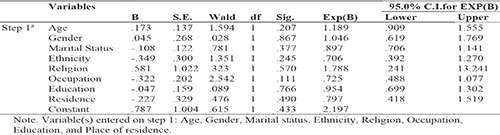
Table 6: A Binary Logistics Regression Analysis of Caregiver's Level of Expressed Emotion on Socio-Demographic Characteristics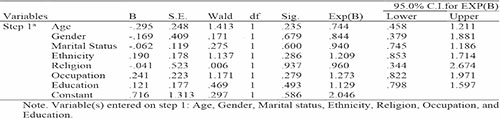
Binary logistic regressions (Tables 5 and 6) revealed that neither patient nor caregiver socio-demographic variables significantly predicted the caregiver’s level of expressed emotion (all p > .05). This encompasses factors such as age, gender, marital status, ethnicity, religion, occupation, education, and place of residence.
Section 3: Prevalence of High EE
The study, using the Family Questionnaire (FQ), assessed High-Expressed Emotion (EE) in caregivers of patients with schizophrenia and bipolar disorder at Aminu Kano Teaching Hospital (AKTH). In Table 7, among 250 caregivers, 105 (42.0%) exhibited high levels of expressed emotion, with 145 (58.0%) showing low levels, indicating a significant portion expressing heightened emotion through critical comments. Table 8 shows that out of 250 caregivers, 102 (40.8%) had High EE related to Emotional Over-involvement. Using a median score of 16, Table 9 demonstrates that out of 250 caregivers, 107 (42.8%) had High EE, emphasizing significant criticism and emotional over-involvement towards relatives with severe mental illnesses.
Table 7: Prevalence of High-Expressed Emotion on Critical Comments in Caregivers of Patients with Schizophrenia and Bipolar Disorder at AKTH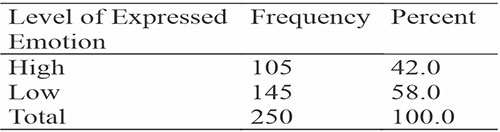
Table 8: Prevalence of High Expressed Emotion on Emotional Over-involvement in Caregivers of Patients with Schizophrenia and Bipolar Disorder at AKTH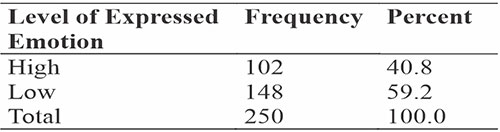
Table 9: Prevalence of High Expressed Emotion in Caregivers of Patients with Schizophrenia and Bipolar Disorder at AKTH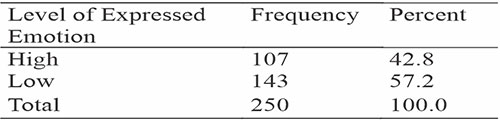
Section 4: Relationship with Personality Traits
The study utilized the Big Five Inventory-2 Short Form (BFI-2-S) to measure the five major dimensions of personality. In Table 10, caregivers of patients with schizophrenia and bipolar disorder at AKTH showed similar mean scores across the five personality traits, suggesting a stable average level of each trait. The correlation matrix in Table 11 indicates that neuroticism had a significant positive correlation with EE, while other personality traits did not significantly influence the emotional climate of the caregiver-patient relationship.
Table 10: Personality Traits of Caregivers for Patients with Schizophrenia and Bipolar Disorders at AKTH: Mean, Median, Mode, and Standard Deviation Scores
Table 11: Correlation Matrix of Expressed Emotions and Personality Traits of Caregivers of Patients at AKTH
Table 12 highlights prevalent trends in caregivers' personality traits from the Big Five Inventory. Logistic regression in Table 13 did not reveal statistically significant associations between caregivers' Big Five personality traits and their level of expressed emotion. Similarly, Table 14 shows that none of the personality traits significantly predicted the level of critical comments.
Table 12: Distribution of Caregivers' Personality Trait Levels with the Big Five Inventory
Table 13: A Binary Logistic Regression Analysis: Predicting Caregivers' Expressed Emotions from Personality Traits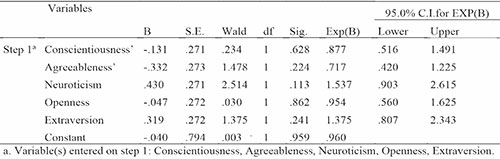
Table 14: Regression Analysis of Caregivers' Personality Traits on Critical Comments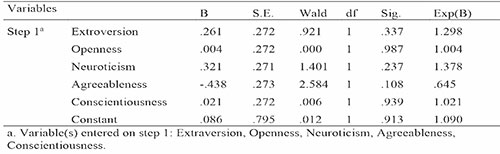
Table 15 presents the binary logistic regression exploring the link between caregivers' level of emotional over-involvement and their Big Five personality traits. None of the personality traits significantly predicted emotional over-involvement, indicating no reliable association between caregivers' tendencies and their personality characteristics.
Table 15: Regression Analysis of Caregivers' Personality Traits on Emotional Overinvolvement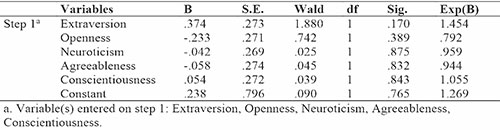
Section 5: Relationship with Patients’ Illness Characteristics
Examining the correlations between expressed emotion (EE) and patients' illness characteristics at AKTH, results in Table 16 show a significant negative correlation (r = -.126, p < .05) between EE and the type of illness. Caregivers of patients with bipolar disorder tended to have lower EE than those with schizophrenia. No other significant correlations were found with illness duration, orthodox treatment, or relapse, indicating independence from these factors.
Table 16: Distribution of Patients' Types of Illness among Caregivers at AKTH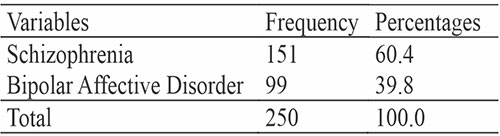
Table 17 provides an overview of the illness characteristics of patients, with 60.4% diagnosed with schizophrenia and 39.8% with Bipolar Affective Disorder, reflecting the prevalent mental health conditions at AKTH. The table also reports patients' relapse and hospitalization durations.
Table 17: Illness Characteristics of Patients Whose Caregivers Were Assessed for High Expressed Emotion at AKTH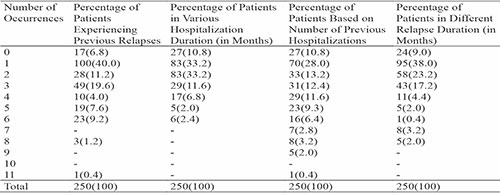
Additionally, Table 18 presents the logistic regression results of EE on patients' illness characteristics. None of the illness characteristics significantly predicted EE (all p > .05), suggesting that patients' illness characteristics did not influence the emotional climate of the caregiver-patient relationship. The model had moderate accuracy (58.4%) in classifying EE levels, with better performance for low (92.4%) than high (19.0%) levels. However, the model's fit was poor, as indicated by low R Square values and non-significant omnibus tests.
Table 18: Regression Analysis of Caregivers' Level of Expressed Emotions and the Patient Illness Characteristics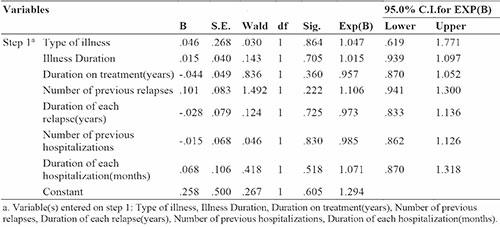
Discussion
This study investigated the prevalence and predictors of Expressed Emotion (EE) among caregivers of patients with schizophrenia or bipolar affective disorder in Kano, Nigeria. EE is a measure of the emotional climate in the family or caregiving environment of a patient with a major mental disorder. High EE, characterized by criticism, hostility, or emotional over-involvement, has been linked to increased relapse risk in various mental conditions, such as schizophrenia, mood disorders, eating disorders, dementia, and autism.8-10 However, most of the existing literature on EE and its predictors is based on Western samples, and there is a dearth of research on EE in the African context.1,2,18 This study aimed to fill this gap by exploring the socio-demographic, personality, and patient-related factors associated with high EE among caregivers in Kano, Nigeria.
The study used a descriptive cross-sectional design with 250 participants selected by systematic random sampling. The participants were adults with schizophrenia or bipolar disorder and their caregivers attending the psychiatric clinic of Aminu Kano Teaching Hospital. Data collection included questionnaires and interviews on socio-demographics, illness characteristics, personality traits, and EE. The study found that the overall prevalence of high EE was 42.8%, with emotional over-involvement being the most common indicator. The study also found that only neuroticism, a personality trait, showed a significant positive correlation with EE, while the other personality traits (extraversion, openness, agreeableness, and conscientiousness) did not predict EE. Furthermore, the study found a significant negative correlation between EE and the type of illness, indicating that caregivers of patients with bipolar disorder had lower EE than caregivers of patients with schizophrenia.
The prevalence of high expressed emotion (EE) in this study (42.8%) is like rates reported in previous studies in Nigeria13,15,23 and Ethiopia2 but is lower than in some regions, such as southern Nigeria,12,22 Egypt,17 and England.8 This suggests differences in EE expression among caregivers influenced by cultural, social, or environmental factors. Hashemi and Cochrane discussed how EE’s meaning and effects vary across cultures and the need for appropriate measurements. They mentioned studies comparing British Asian families and the different ways of coping with mental illness.8 Bhugra and McKenzie emphasized the importance of considering EE in cultural contexts, with different normal rates across cultures, and the need for baseline data before interventions in diverse settings.25
Neuroticism is identified as the sole personality trait correlating with, but not predicting, Expressed Emotion (EE), consistent with prior research.20,21 Booker contrasts the positive impact of extraversion with the detrimental effect of neuroticism on caregiver health.21 Amaresha and Venkatasubramanian explore various factors influencing caregiver EE in schizophrenia, including optimism, self-efficacy, empathy, patience, beliefs about illness causes, controllability, and guilt feelings.1 Hooley and Hiller's study on high-EE relatives reveals patterns of conventional behaviour, diminished life satisfaction, reduced flexibility and tolerance, and lower empathy and achievement via independence. These insights emphasize the complexity of EE, necessitating tailored interventions and ongoing research. Integrating personality considerations into EE studies is crucial for advancing clinical applications and future investigations.20
The finding that caregivers of patients with bipolar disorder exhibited lower expressed emotion (EE) compared to caregivers of patients with schizophrenia aligns with prior studies reflecting a consistent pattern.15,27,28-30 This observed distinction may be attributed to differences in symptoms, course, and prognosis between the two disorders, influencing caregivers' expectations, attitudes, and coping strategies. Notably, some studies propose that caregivers of individuals with bipolar disorder may demonstrate higher levels of hope, optimism, and acceptance than caregivers of those with schizophrenia, potentially contributing to the observed lower EE.27,29
The findings from the study present crucial insights into the relationship between caregivers' expressed emotions (EE) and various patient illness characteristics. In comparison to studies conducted in other regions,1,2,5,17,18,22,23 our results challenge conventional assumptions about the influence of specific illness attributes on the emotional climate within caregiver-patient relationships. It suggests that, at least within the studied population in Kano, Nigeria, factors other than those examined in the analysis play a more prominent role in shaping caregiver EE.
The non-significant associations could imply a greater complexity in the caregiver-patient dynamic, potentially influenced by cultural, social, or individual factors not accounted for in the current analysis. Additionally, it prompts further exploration into the specific contextual elements that contribute to the expression of emotions among caregivers in this region.
This finding aligns with the broader literature on expressed emotion, emphasizing the need to consider diverse factors beyond traditional illness characteristics when understanding the emotional dynamics between caregivers and individuals with major psychiatric disorders.19-21,25 The results of this study contribute to a detailed understanding of caregiver-patient relationships in the context of mental health in Kano, Nigeria, challenging existing assumptions and paving the way for more comprehensive investigations into the multifaceted nature of expressed emotions.
Strengths and limitations
This study benefits from a robust design, featuring a large and representative sample. Validated instruments for measuring Expressed Emotion (EE) and personality enhance the credibility and comprehensiveness of findings. The inclusion of both patients and caregivers as participants further strengthens the study.
The study's cross-sectional nature limits the establishment of causal relationships between variables. Future longitudinal or experimental studies are essential for understanding the direction and magnitude of effects related to personality, illness type, and other factors on EE. Reliance on self-report measures may introduce biases or errors related to social desirability, recall, or response styles. Utilizing objective or observational measures for EE and personality could yield more accurate and reliable data. The study did not account for potential confounding variables, such as illness duration and severity, the quality and frequency of patient-caregiver contact, and the availability/utilization of mental health services. Future research should consider these factors for a more comprehensive analysis.
Conclusion
This study investigated the prevalence and predictors of expressed emotion (EE) among caregivers of patients with severe mental illnesses (SMIs) in Nigeria. The results showed that high EE was prevalent among the caregivers and that though correlated with neuroticism, it did not predict personality traits. EE was related to illness type. Caregivers of patients with schizophrenia and those with higher levels of neuroticism and lower levels of agreeableness and conscientiousness were more likely to exhibit high EE. These findings suggest that personality and illness type are important factors to consider in understanding and addressing EE among caregivers of SMI patients in Nigeria. The study also highlighted some of the strengths and limitations of the research design and methods and offered some recommendations for future research in this area. The study contributes to the existing literature on EE and its correlates in African settings and provides implications for clinical practice and policy.
Recommendations for future research
Based on the findings and limitations of this study, some recommendations for future research can be made. First, more studies are needed to explore the prevalence and predictors of EE in different African contexts and to compare them with the findings from Western and other non-Western settings. This will help to understand the cultural and contextual influences on EE and its implications for mental health outcomes. Second, more studies are needed to examine the mechanisms and processes through which personality and illness type affect EE, and how these factors interact with each other and with other variables. This will help to identify the modifiable and non-modifiable factors that can be targeted for intervention to reduce EE and improve the quality of life of patients and caregivers. Third, more studies are needed to evaluate the effectiveness and feasibility of interventions to reduce EE among caregivers in Africa and to identify the best practices and strategies for implementing them. This will help to bridge the gap between research and practice and to provide evidence-based and culturally appropriate solutions for the challenges faced by caregivers of patients with severe mental illnesses.
References
- Amaresha AC, Venkatasubramanian G. Expressed emotion in schizophrenia: an overview. Indian J Psychol Med. 2012 Jan;34(1):12-20.
- Yimam B, Sobotka M, Getachew Y, Alemu B, Ahmed G, Tesfaye E, Necho M. High expressed emotion among caregivers of schizophrenic patients in Southwest Ethiopia: a comprehensive study. Ann Gen Psychiatry. 2022; 21:27.
- Brown GW. The discovery of expressed emotion: Induction or deduction? In: Leff J, Vaughn C, editors. Expressed Emotion in Families. New York: Guilford Press; 1985. pp. 7–25.
- Leff J. The concept of expressed emotion: new empirical evidence. World Psychiatry. 2018; 17(1): 3-4.
- Wearden AJ, Tarrier N, Barrowclough C, Zastowny TR, Rahill AA. A review of expressed emotion research in health care. Clin Psychol Rev. 2000; 20:633–66.
- Parker G, Hadzi-Pavlovic D, Roussos J, Wilhelm K, Mitchell P, Austin MP, Hickie I. Expressed emotion: a comparison of the Camberwell Family Interview and the Five-Minute Speech Sample. Acta Psychiatr Scand. 1997; 95(6):508-13.
- Dodd CG, Schoonover CE. Camberwell Interview for Assessing Expressed Emotion in Families. In: Lebow JL, Chambers AL, Breunlin DC, editors. Encyclopedia of Couple and Family Therapy. Cham: Springer; 2018
- Hashemi AH, Cochrane R. Expressed emotion and schizophrenia: a review across cultures. Int Rev Psychiatry. 1999; 11:219-224.
- Tyagi A, Choudhary S, Deep R. Expressed emotion in psychiatric disorders: A review. Indian J Soc Psychiatry. 2017;33(1):3-10
- Baby Shalini, John SA, Sebastian J. A study to assess the expressed emotion among caregivers of patients with psychiatric disorders. IOSR J Nurs Health Sci. 2022;11(4):40-50
- Toshiyuki K, Motoichiro K, Robert R. The low prevalence of high expressed emotion in Bali. Psychiatr Res. 2000;94(3):229-238.
- Christian E. Case studies of family expressed emotion for families of patients living with schizophrenia in Delta State of Nigeria. Eur J of Mental Health. 2009;4(2):247-252.
- Ogbolu RE, Adeyemi JD, Erinfolami AR. Expressed emotion among schizophrenic patients in Lagos, Nigeria: A pilot study. Afr J Psychiatry. 2013;16(5):329-331
- Carra G, Cazzullo CL, Clerici M. The association between expressed emotion, illness severity and subjective burden of care among relatives of patients with schizophrenia: findings from an Italian population. BMC Psychiatry. 2012;12(140).
- Ayilara O, Ogunwale A, Babalola E. Perceived expressed emotions among relatives of patients with severe mental illness: A comparative study. J Psychiatr Res. 2017;257:137-143.
- Greenly JR. Social control and expressed emotion. J Nerv Ment Dis. 1986; 174:24-30.
- Kamal A. Variables in expressed emotion associated with relapse: A comparison between depressed and schizophrenia patients in an Egyptian community. Curr Psychiatry.
- Ola BA. The influence of burden of care and perceived stigma on expressed emotions of relatives of stable persons with schizophrenia in Nigerian semi-urban/urban settings [thesis]. Lagos: University of Lagos; 2013.
- Barrowclough C, Johnston M, Terrier N. Attributions, expressed emotion and patient relapse. An attribution model of relatives’ response to schizophrenia illness. Behav Ther. 1994; 25:67-88.
- Hooley JM, Hiller JB. Personality and expressed emotion. J Abnorm Psychol. 2009; 109:40-4.
- Booker K. Caregiver personality traits affect mental and physical health [Internet]. Cornell Chronicle. 2011 [cited 2023 Dec 15]. Available from: https://news.cornell.edu/stories/2011/09/personality-traits-affect-caregivers-health
- Reitcher B, Adeyemi JD, Lawal RA, Famuyiwa OO, Haruna AY, Jibodu MO. The emotional reaction of relatives of schizophrenic patients in Lagos. Afr J Med Med Sci. 2003;32(1)
- Babandi F, Usman UM, Habib ZG, Owolabi DS, Gudaji MI, Taura AA, Aghukwa CN, Baguda AS, Salihu AS. Caregiver Expressed Emotion, Quality of Life, and Medication Adherence among People Living with Schizophrenia in Nigeria. J Biomed Res Environ Sci. 2022;3:627-633.
- Wiedemann G, Rayki O, Feinstein E, Hahlweg K. The Family Questionnaire: development and validation of a new self-report scale for assessing expressed emotion. Psychiatry Res. 2002;109(3):265-279
- Bhugra D, McKenzie K. Expressed emotion across cultures. Adv Psychiatr Treat. 2003;9(5):342-348.
- Costa PT Jr, McCrae RR. The Revised NEO Personality Inventory (NEO-PI-R). In: Boyle GJ, Matthews G, Saklofske DH, editors. The SAGE Handbook of Personality Theory and Assessment, Vol. 2. Personality Measurement and Testing. Sage Publications, Inc.; 2008. p. 179–198.
- Reinares M, Vieta E, Colom F, et al. What really matters to bipolar patients’ caregivers: sources of family burden. J Affect Disord. 2006;94(1-3):157-163.
- Perlick DA, Rosenheck RA, Miklowitz DJ, et al. Prevalence and correlates of burden among caregivers of patients with bipolar disorder enrolled in the Systematic Treatment Enhancement Program for Bipolar Disorder. Bipolar Disord. 2007;9(3):262-273.
- Perlick DA, Hohenstein JM, Clarkin JF, et al. Factors associated with expressed emotion ratings among parents of bipolar adolescents. J Am Acad Child Adolesc Psychiatry. 2005;44(1):28-36.
- Perlick DA, Miklowitz DJ, Lopez N, et al. Family-focused treatment for caregivers of patients with bipolar disorder. Bipolar Disord. 2010;12(6):627-637.