Early childhood caries among pre-school children in rural areas
Osadolor OO1, Osadolor AJ2,3
Abstract
Background: Early childhood caries can occur and exist among children in slums areas, rural areas and under-served communities. Africa has countries with rural areas inhabited by diverse ethnic populations of pre-school children, with their parents and family members.
Method: An electronic literature search in Science direct and PubMed was done in January, 2024 using the Population, Concept and Context framework. Search terms and keywords were combined by Boolean operators. Two independent investigators screened titles and abstracts of publications on early childhood caries among pre-school children in rural areas. The inclusion criteria was original (primary) research articles with accessible full text, related to early childhood caries among pre-school children in rural areas, carried out in Africa, published in English and in electronic databases. Original research articles related to early childhood caries among pre-school children in urban, semi-urban or sub-urban areas, hospital based studies, studies with participants selected from rural and urban or rural and semi-urban communities, review articles, systematic reviews, thesis or dissertations were excluded during screening.
Results: Three articles with accessible full texts were included as it was assessed to meet the aim of the review. The study designs of the included studies were cross-sectional study, randomized, controlled field trial and a case-control study respectively. The studies were carried out in rural areas of Uganda and Egypt respectively.
Conclusion: Early childhood caries has multifactorial aetiology. More studies from diverse ethnic population in Africa countries will fill the gaps in knowledge and add to the existing literature.
Keywords: Africa, Children, Early childhood, Rural, Studies
Introduction
Early childhood caries (ECC) according to the definition of The American Academy of Paediatric Dentistry (AAPD) is the presence of one or more decayed (non-cavitated or cavitated lesion), missing (due to caries), or filled tooth surfaces in any primary tooth in a child, 71 months of age or younger.1-5 Early childhood caries is considered to be severe when there is presence of smooth-surface caries in children younger than three years of age, when there is presence of one or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth for children ages 3 - 5 years or a dmft score ≥ 4 (for 3 years), a dmft score ≥ 5 (for 4 years) or a dmft score ≥ 6 (for 5 years).3,6 Studies on early childhood caries had been reported from Spain,7 Brazil,8 Iran,9 Poland,10 Saudi Arabia,11 Cambodia,12 Sweden,13 india14 and other countries globally. In Africa, studies on early childhood caries had been reported from Tunisia,15,16 Uganda,17,18 Tanzania,18,19 South Africa,20 Egypt,1,21-23 Kenya,24,25 Nigeria2,3,5,6,26 and other Africa countries. The aim of this article is to review the available studies on early childhood caries among pre-school children in rural areas in Africa.
Literature search method
An electronic literature search in PubMed and Science direct was done in January, 2024 using the Population, Concept and Context framework.27
Population: Pre-school children
Concept: Early childhood caries among pre-school children in rural areas.
Context: Studies carried out in Africa continent, published in English language and in electronic
databases
The keywords used were early childhood caries, rural, Sub-Saharan countries, pre-school children, Africa countries, primary teeth, African children and Africa. Search terms and keywords were combined by Boolean operators. The inclusion criteria were original (primary) research articles with accessible full text, related to early childhood caries among pre-school children in rural areas, conducted in Africa, published in English and in electronic databases. Original research articles related to early childhood caries among pre-school children in urban, semi-urban or sub-urban areas, hospital based studies and studies with participants selected from rural and urban or rural and semi-urban communities were excluded. Review articles, systematic reviews, thesis, viewpoints, books, letters, editorials, dissertations, book chapters, primary study without accessible full text, perspectives, and news related to early childhood caries among pre-school children in rural areas were excluded. Two independent investigators screened titles and abstracts of publications on early childhood caries among pre-school children in rural areas studies, and potential references to identify which studies met the inclusion criteria of this review. Information was extracted from the full texts of articles regarding the location of the research and the main content. Study data of the included articles were extracted and collated in a table, including study details (author(s), year of publication, study population, study location or country, study objectives, study design). All identified studies in Africa that met the inclusion criteria with accessible full text was included and if relevant data were missing, the authors of the articles were not contacted for additional information via e-mail and no specified time frame was used during the search.
Results
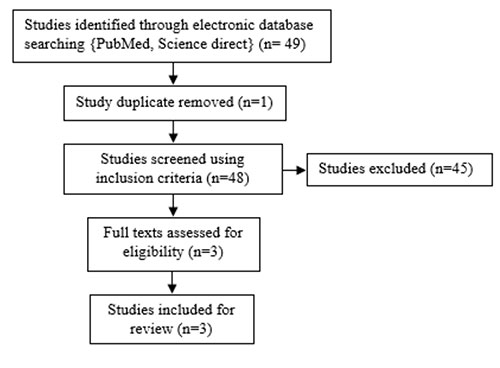
Figure 1: Flowchart of articles process
Table 1: Summary of identified study on early childhood caries among rural pre-school children in Africa countries
Forty nine articles were identified; one duplicate was removed during screening. Abstract and full text was screened using inclusion criteria by two independent investigators. Forty five articles were excluded because they did not meet the inclusion criteria. Three articles with accessible full texts were included as they were assessed to meet the aim of the review. The study designs of the included studies were randomized, controlled field trial, cross-sectional study, and case-control study respectively. The studies were conducted in rural areas of Uganda and Egypt respectively
Discussion
Dental caries is a biofilm mediated, diet modulated/sugar driven, multifactorial, dynamic28 oral disease. The prevalence of early childhood caries varies from country to country and region to region28 as a result of various socio-cultural and multifactorial factors. In Uganda, the prevalence of early childhood caries among 3-5 years old rural pre-school children was 48.6%,17 with a prevalence of 11.6%, 18.5% and 18.5% among 3-, 4-, and 5-year old children, respectively.17 Early childhood caries was seen more in males than females17. The finding of 48.6% was greater than previous report of 3.7% among 6-36 months old children in Tanzania,18 greater than previous report of about 25.2%21 among 1-3 years rural Egyptian pre-school children and less than 54.5%13 among 18-36 months old rural children in Cambodia and 52%16 among 1-5 year old children in rural area in Tunisia respectively. This variation could be as a result of the differences in age of the study participants as early childhood caries is a multifactorial dynamic oral disease that occurs over a period of time.
Early childhood caries is a multifactorial oral disease1-3,5,6 that involves a susceptible tooth surface, fermentable carbohydrates, cariogenic microorganisms5 (Streptococcus mutans, Lactobacili spp) and a period of time. Risk factors1-3,6 associated with early childhood caries initiation and progression include socio-demographic factors like age, parents’ level of education, parents’ occupation and child birth rank. Biological factors1 like salivary pH, buffering capacity of saliva, saliva flow rate, re-mineralising ions present in saliva, saliva viscosity and dietary factors like breast/bottle feeding, night feeding, frequency of intake of sugary snacks, and oral-health related behaviours1 like frequency of tooth brushing, oral hygiene practices, dental visits and use of fluoride containing toothpaste.
A study from Egypt reported that age, mother’s education, frequency of daily sugary snacks, night feeding, and oral health status are possible risk factors for early childhood caries in rural areas1. This finding reflects the multifactorial factors associated with the initiation and progression of early childhood caries. Another study from Egypt reported23 that combination of 38% Silver Diamine Fluoride (SDF, (44,800 ppm) with 5% sodium fluoride (NaF, 22 600 ppm) varnish had better arrest of early childhood caries lesions than use of 38% Silver Diamine Fluoride (SDF) alone and the difference was significant in moderate carious lesion (assessed using International Caries Detection and Assessment System criteria) but not advanced carious lesions. Silver diamine fluoride29 and fluoride varnish are among the non- invasive methods (like use of calcium and phosphate containing re-mineralising agent like casein phosphopeptide-amorphous calcium phosphate) for managing early lesion of early childhood caries and fluoride is among the World Health Organization model list of essential30 medicine for children.
Conclusion
Early childhood caries is a significant public health problem with multifactorial aetiology. Rural community based oral health awareness (targeting parents, family members and guardians) programme/activities on the benefits of reducing intake of cariogenic diets like biscuits among pre-school children, twice daily tooth brushing of teeth with fluoride containing toothpaste (smear (0.1mg fluoride) for children under 3 years, or pea (0.25mg fluoride) size for 3-6 years old children) by the parents/guardians, reduction of nocturnal breastfeeding and bottle feeding habits and improvement of oral health seeking behaviour of the parents could reduce the prevalence of early childhood caries among children in rural areas. Africa has about 3000 ethnic groups with various socio-cultural practices and beliefs. More studies from diverse rural ethnic population in Africa will fill the gaps in knowledge and add to existing literature.
Financial support and sponsorship
None
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
Authors acknowledge all advisers of this article.
References
- Attia D, ElKashlan MK, Saleh SM . Early childhood caries risk indicators among preschool children in rural Egypt: a case control study BMC Oral Health 2024; 24:10.
- Oziegbe EO, Schepartz LA. Parity, Maternal-Child Oral Interactions and Early Childhood Caries (ECC) among Northern Nigerian Hausa children. Dental Research and Oral Health. 2023;6: 28-39.
- Onyejaka NK, Amobi EO. Risk factors of early childhood caries among children in Enugu, Nigeria. Brazilian Research in Pediatric Dentistry and Integrated Clinic 2016;16(1):381-391.
- American Academy of Pediatric Dentistry. Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. The reference Manual of Pediatric Dentistry. Chicago, Ill.: American Academy of Pediatric Dentistry; 2020:79–81.
- Iyun OI, Denloye OO, Bankole OO, Popoola BO. Mutans streptococci colonization in early childhood caries in Ibadan, Nigeria. Pediatric Dental Journal 2014;24:153-158.
- Olatosi OO, Inem V, Sofola OO, Prakash P, Sote EO. The prevalence of early childhood caries and its associated risk factors among preschool children referred to a tertiary care institution. Niger J Clin Pract 2015;18(4):493-501.
- Carrillo-Díaz M , Ortega-Martínez AR., Ruiz-Guillén A, Romero-Maroto M., González-Olmo MJ. Impact of Breastfeeding and Co sleeping on Early Childhood Caries: A Cross-Sectional Study. J. Clin. Med. 2021;10:1561.
- Lotto M, Strieder AP, Aguirre PE, Oliveira TM, Machado MA, Rios D et al. Parental-oriented educational mobile messages to aid the control of early childhood caries in low socioeconomic children: A randomized controlled trial. Journal of Dentistry 2020; 101: 103456.
- Javadzadeh E, Razeghi S, Shamshiri A, Miri HH, Moghaddam F, Schroth RJ, et al. Prevalence and socio-behavioral determinants of early childhood caries in children 1–5-year-old in Iran. PLoS ONE 2023; 18(11): e0293428.
- Olczak-Kowalczyk D, Gozdowski D , Turska-Szybka A . Protective Factors for Early Childhood Caries in 3-Year-Old Children in Poland. Front. Pediatr.2021; 9:583660.
- AlMarshad LK, Wyne AH, AlJobair AM. Early childhood caries prevalence and associated risk factors among Saudi preschool children in Riyadh Saudi Dental Journal 2021; 33:1084–1090.
- Boustedt K, Roswall J, Kjellberg E, Twetman S, Dahlgren J. A prospective study of perinatal and metabolic risk factors for early childhood caries. Acta Paediatr. 2020;109:2356–2361.
- Kubota Y, San Pech N, Durward C, Ogawa H. Association between Early childhood caries and maternal factors among 18 to 36 months old children status in a rural area of Cambodia. Oral Health Prev Dent. 2020;18:973-980.
- Phogat R, Rani G, Manjunath BC, Kumar A, Rani V. Relationship of anthropometric measurements and nutritional status with early childhood caries among rural preschool children – A cross sectional analytical study. J Indian Assoc Public Health Dent 2023; 21:306 12.
- Chouchene F, Masmoudi F, Baaziz A, Maatouk F and Ghedira H. Early Childhood Caries Prevalence and Associated Risk Factors in Monastir, Tunisia: A Cross-Sectional Study. Front. Public Health 2022; 10:821128.
- Chamli MA, Chouchene F, Benzineb Taher I, Masmoudi F, Baaziz A, Maatouk F et al. Prevalence of Early Childhood Caries and Its Associated Risk Factors Among Preschool Children in Sousse: A Cross-Sectional Survey. J Pediatr Dent 2020;6(2):39-45.
- Musinguzi N, Kemoli A, Okullo I. Prevalence and Treatment Needs for Early Childhood Caries Among 3–5-Year-Old Children From a Rural Community in Uganda. Front. Public Health 2019; 7:259.
- Masumo R, Bardsen A, Mashoto K, Åstrøm AN. Prevalence and socio-behavioral influence of early childhood caries, ECC, and feeding habits among 6 – 36 months old children in Uganda and Tanzania BMC Oral Health 2012;12:24.
- Ndekero TS, Carneiro LC, Masumo RM. Prevalence of early childhood caries, risk factors and nutritional status among 3-5-year-old preschool children in Kisarawe, Tanzania. PLoS ONE 2021; 16(2): e0247240.
- Mohamed N, Barnes JM. ‘Early childhood caries and dental treatment need in low socio-economic communities in Cape Town, South Africa’, Health SA Gesondheid 2018; 23:a1039.
- Bastawy A, Barakat I. Potential Impact of Dietary Habits, Body Mass Index and Family Function on Early Child Hood Caries Among 12 to 36 Month-Old Children in A Rural Area of Egypt. AADJ 2023;6:73-85.
- Quritum M , Abdella A, Amer H ,El Tantawi M. Effect of silver diamine fluoride and nano silver fluoride on oral health-related quality of life of children with early childhood caries: A randomized clinical trial. Journal of Dentistry 2024;142: 104878.
- Abdellatif EB, El Kashlan MK, El Tantawi M. Silver diamine fluoride with sodium fluoride varnish versus silver diamine fluoridein arresting early childhood caries: a 6-months follow up of a randomized field trial BMC Oral Health 2023; 23:875.
- Njoroge NW, Kemoli AM, Gatheche LW. Prevalence and pattern of early childhood caries among 3-5 year olds in KIAMBAA, KENYA East African Medical Journal 2010; 87(3) :134-137.
- Njoroge NW, Kemoli AM, Gatheche LW. Early childhood caries amongst pre-school children and their caregivers’ perceptions of oral health in a Kenyan rural setting. East African Medical Journal 2015; 92(8) : 389-393.
- Alade M, Folayan MO, El Tantawi M3, Oginni AB, Adeniyi AA, Finlayson TL Early childhood caries: Are maternal psychosocial factors, decision-making ability, and caries status risk indicators for children in a sub-urban Nigerian population? BMC Oral Health 2021;21:73.
- Osadolor OO. Hall technique for the management of carious primary molar teeth among African children-a review. IMC. J. Med. Sci.2024; 18(1):003.
- Global oral health status report towards universal health coverage for oral health by 2030.Geneva: World Health Organization;2022:30-36.
- Osadolor OO . Acceptability of Silver Diamine Fluoride. Journal of Rangpur Medical College. 2023;8(2):53-55.
- Gkekas A, Varenne B, Stauf N, Benzian H, Listl S. Affordability of essential medicines: The case of fluoride toothpaste in 78 countries. PLoS ONE 2022; 17(10): e0275111.