Prevalence of musculoskeletal related morbidity and its perceived impact on health among pregnant women in a tertiary centre
Osazee K1, Nnakwe LM2, Iribhogbe OI2
Abstract
Background: Pregnancy is a physiological condition associated with musculoskeletal symptoms of which the site, perception, severity, effect on the quality of life and treatment vary in individuals.
Objective: To determine the prevalence of musculoskeletal morbidity, its relationship with socio-clinical characteristics, perception, and impact on the quality of life of pregnant women attending antenatal clinics at the University of Benin Teaching Hospital.
Results: Four hundred antenatal women participated in this study; 146 (48.7%) experienced musculoskeletal problems during the index pregnancy. Most respondents (51.3%) were 31-40 years (mean 31.9±5.6). For those who experienced problems, the onset of symptoms was highest (49.3%) in 3rd trimester, and the majority (76%) had tertiary education. The most typical problem was pelvic pain (48.8%); the most common predisposing factor was previous trauma (100%). Most (72.6%) perceived symptoms as moderate pain that affected their quality of life. Treatment was majorly rest (47.5%), 59.4% had their symptoms relieved, and 76.3% were satisfied with their treatment.
Conclusion: This study showed a prevalence of approximately 50%, with the commonest predisposing factor being previous trauma and pelvic pain being the most common problem. Therefore, Clinicians should be aware of the musculoskeletal problems in otherwise healthy pregnant women and manage them appropriately.
Keywords: Musculoskeletal, Pregnancy, Antenatal
Introduction
Pregnancy is a physiological condition associated with marked changes in all body organ systems, including the musculoskeletal system.1,2 The changes that occur in Pregnancy are part of an adaptive mechanism to enable the woman to accommodate the Pregnancy and prepare for the process of parturition.3 The changes arise from elevated hormone concentration and physical changes in Pregnancy.1-4 During Pregnancy, the process of preparing the pelvis for delivery involves hormones such as progesterone and relaxin that cause general laxity and softening of ligaments and joints, which to a large extent, is the primary reason why many women develop musculoskeletal problems during Pregnancy.3,4 Riahi et al. illustrated imaging characteristics of the main musculoskeletal pelvic disorders during Pregnancy, labour and postpartum. They noted that Pregnancy, with its induced hormonal and physical changes, increases the risk of developing musculoskeletal dysfunction in Pregnancy.4 To this set of women who do not have some of these problems before Pregnancy, there is complete resolution of symptoms postpartum.
Other predisposing factors for the development of musculoskeletal dysfunction during Pregnancy include female gender, genetic predisposition, advanced maternal age, previous pelvic trauma, history of musculoskeletal dysfunction at an earlier Pregnancy, multiparity, raised body mass index, strenuous work/job, emotional distress.1-7.
The prevalence of musculoskeletal disorders in Pregnancy varies globally and is influenced by factors like level of activity, job/occupation, cultural influences, environment, age, and parity.8,9 A prevalence of 67% was reported in the United States,10 50.7% in India,8 and 55.7% in Southeast Nigeria.1 While 53.8% among non-pregnant women in Benin.12 There is a paucity of literature on the prevalence of musculoskeletal disorders in Pregnancy in Benin City.
Work-related musculoskeletal dysfunction in Pregnancy has been noted to occur more in women who do strenuous jobs or repeated exposure to forceful and prolonged physical activities or awkward postures like long hours of standing, much bending and lifting of heavy objects.6,13,14
Various factors like culture, religion, ethnicity, and level of education influence the perception and expression of musculoskeletal pain during Pregnancy or labour.15 Social scientists have reported strong associations of culture with pain responses, beliefs, and behaviour.16,17 In some cultures, women are made to anticipate and cope with pregnancy and labour pains as a normal physiological event which is short-lived postpartum; otherwise, they will be seen as a weakling.15 This is even with moderate pains that had been shown to persist in 10% of patients postpartum14-18 Evidence have shown that Muslims had lower pain perception than Christians.17,18 This may reflect religious or cultural values that influence the expression of pain as Muslim women, mainly from northern Nigeria, rarely screen for pain during labour.18-20.
Almost all joints and muscles in the body can be affected by Pregnancy; however, commonly reported musculoskeletal problems in Pregnancy are low back pains, pelvic girdle pain, hip pain, thigh pain and knee pain.2,20 Others are Leg cramps, foot pain, hand/wrist pain, and chest and abdominal pains.21 Of these common complaints, the low back appears to be the most common complaint, accounting for over 50%.20,21
Musculoskeletal symptoms in Pregnancy are attributed to the effects of hormones during Pregnancy and the consequences of gravity and the gravid uterus.19,21 Elevated concentrations of hormones like progesterone, oestrogen and relaxin cause ligamentous laxity, hypermobility of the joints and fluid retention during Pregnancy.22 This laxity of the ligaments leads to alteration in pelvic architecture and widening of the symphysis pubis to allow for childbirth.22 The enlarging gravid uterus causes Lumber hyperlordosis, contributing to the mechanical strain on the back and sacroiliac joints.23 It also stretches and splits the anterior abdominal wall (Recti abdominis diastasis), which alters the neutral position by anteriorly shifting the center of gravity.24 The enlarging uterus, together with weight gain, constitutes mechanical stress on the body /joints.1,23,24
Emerging evidence has shown that complaints related to musculoskeletal disorders in Pregnancy are one of the most distressful conditions pregnant women often present with during their antenatal clinic visits, yet it gets the least attention from the managing Physicians;25,28-32 and the Physician cannot overrule the impact of musculoskeletal disorders in their quality of lives. This physical dysfunction, poor work performance and absence from work tend to reduce the productive efficiency of these women, thereby affecting the economy of the family, the community and the state in general.26,27,33-35
Managing musculoskeletal disorders in Pregnancy is essential for any woman during Pregnancy and postpartum to prevent chronic musculoskeletal problems, promote both physical/social well-being and prolong life.22,24,34 Commonly, most musculoskeletal disorders are self-limiting and can be managed conservatively by postural training, exercise, rest, massaging, increased hydration and warm tub bath.22,23,34 However, about 25% of pregnant women experience temporarily disabling symptoms and require management with orthopaedic surgeons, physiotherapist and chiropractic.35,36 While obstetricians manage some.35,36 The Physician should seek their satisfaction with the treatment modality for the symptoms.34,36
This study aimed to determine the prevalence of musculoskeletal disorders among pregnant women in the University of Benin Teaching Hospital (UBTH) and the impact of these disorders on health during Pregnancy.
Materials and methods
The study population consisted of all pregnant women who booked and received antenatal care at UBTH during the study period. The sample size was determined using the Cochran formula for sample size determination for a cross-sectional study. Combined Stratified and simple random sampling techniques were used for this study. The researcher and other trained research assistants obtained clinical information from the patients using Interviewer administered open and close-ended questionnaires. The questionnaire contains questions about the patient's demographic and clinical characteristics obtained from the patient's booking records in the department. Relevant aspects of the musculoskeletal disorders adopted from the Nordic Musculoskeletal Questionnaire (NMQ), Roland-Morris Low Back Pain Disability Questionnaire (RMQ), and Pelvic Girdle Pain Questionnaire (PGQ) were administered. The various types of musculoskeletal disorders prevalent among pregnant women were assessed using the components of the Nordic Musculoskeletal Questionnaire. The treatment received for the symptoms, the improvement of the symptoms based on the treatment received and their level of satisfaction with the treatment were also assessed.
Data collected were entered into a statistical package for scientific solution (SPSS) Statistical Software Version-20. The analyzed results were presented in simple frequency tables, percentages, charts, and, where necessary, distributive statistics (mean values ± standard deviation) to describe the population's mean. An association between the social characteristic (age, tribe, level of education, occupation, religion) and clinical characteristics (Parity, gestational age, previous Caesarean/pelvic surgery, prior delivery of macrocosmic baby, trauma) and presence or absence of musculoskeletal disorders, was done such that categorical outcome variables (Impact on health/quality of life, satisfaction with treatment) was analyzed using Chi-square and Fischer's exact test where appropriate. In contrast, continuous variables such as age, weight, occupation, and level of education were analyzed using the student t-test. A P- value of <0.05 was considered statistically significant.
Results
Table 1: Socio-demographic characteristics and BMI of respondents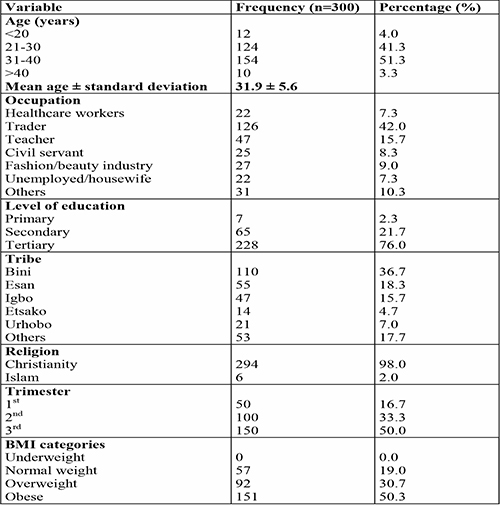
Three hundred antenatal women took part in the study. Fifty of the women were in their 1st trimester, 100 were in their 2nd trimester, and 150 were in their 3rd trimester of Pregnancy.
Table 1: Shows the distribution of socio-demographic characteristics and Body mass index (BMI) of the 300 respondents. Of most respondents, 154(51.3%), 300 were 31-40 years old, with a mean of 31.9±5.6. They were primarily traders 126(42.0%), and 228(76%) had a tertiary level of education. The majority, 110(36.7%), were of the Bini tribe, and 294 were Christians (98%). The prevalence of musculoskeletal problems increased with increasing BMI; 151(50.3%) were obese, while 92(30.7%) were overweight.
Table 2: Clinical characteristics of respondents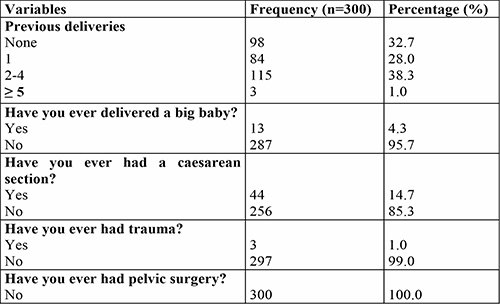
Table 2: Shows the distribution of the clinical characteristics of the 300 respondents. The majority of the respondents, 115(38.3%), were Para 2-4, 13(4.3%) of them had previously delivered a macrosomic baby, 44(14.7%) of them had had caesarean section previously, 3(1%) had trauma previously. None of them had any other pelvic surgery.
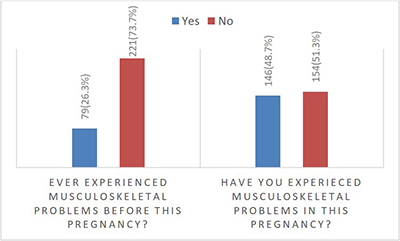
Figure 1: Distribution of respondents who had experienced musculoskeletal problems before current pregnancy and during current pregnancy (n= 300)
Figure 1: Shows the distribution of the respondents who had experienced musculoskeletal problems before the current Pregnancy and in the index pregnancy. Seventy-nine (26.3%) of the respondents experienced musculoskeletal problems before index pregnancy, while 146(48.7%) experienced it in current Pregnancy.
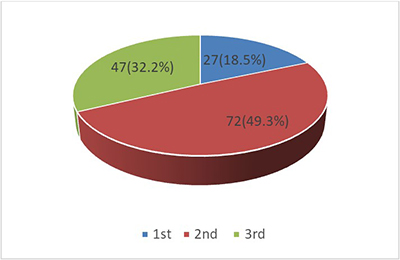
Figure 2: Trimester at the onset of musculoskeletal problems (n=146)
Figure 2: Showed distribution of trimester at the onset of musculoskeletal problems for the 146 respondents who experienced musculoskeletal problems. The onset of musculoskeletal symptoms was mainly in 3rd trimester (49.3%) compared to 2nd and 1st trimesters (32.2% and 18.5%), respectively.
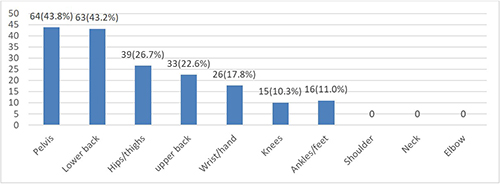
Figure 3: Types of musculoskeletal problems experienced by respondents (Multiple responses) (n=146)
Figure 3: Showed distribution of the types of musculoskeletal problems experienced by respondents. Pelvic pain had the highest prevalence (48.8%) in this study, followed by low back pain (43.2%), with wrist/hand pain being the least (10.3%). None in this study experienced shoulder, neck or elbow pains.
Table 3: Distribution of Socio-demographic and clinical characteristics of respondents who experienced musculoskeletal problems in the index pregnancy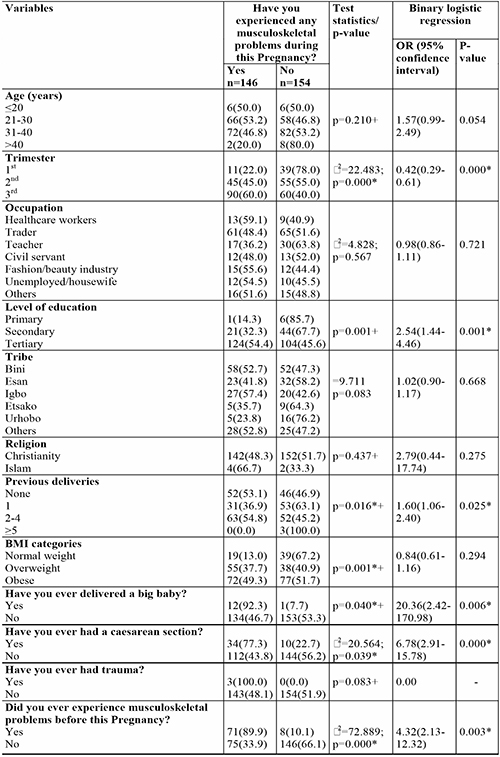
Table 3: Showed the distribution of Socio-demographic and clinical characteristics of respondents who experienced musculoskeletal problems in the index pregnancy. Of the 300 respondents, 146(48.7%) experienced musculoskeletal discomfort during Pregnancy. There was no significant difference in the age of respondents who suffered musculoskeletal problems in index pregnancy; 46.8 % versus 53.2% with a p-value of 0.054 for age groups 31- 40 and 21- 30 years, respectively.
Most respondents experienced musculoskeletal symptoms mostly in their 3rd trimester compared to the 2nd and 1st trimesters; 60% versus 45% versus 22% (p = 0.000), respectively. This shows that the prevalence of musculoskeletal symptoms increases with increasing duration of Pregnancy.
Although the prevalence of musculoskeletal dysfunction was higher among health workers (59.1%) and fashion designers (55.6%), occupation was not significantly associated with complaints of musculoskeletal discomfort (p = 0.721). Level of education was significantly associated with the perception and complaint of musculoskeletal symptoms as 54.4% of respondents with tertiary level of education perceived the pains as against 32.3% and 14.3% with secondary and primary levels of education, respectively (p = 0.001).
In this study, the prevalence of musculoskeletal dysfunction had no association with tribe though the three major tribes in Nigeria were not represented here. However, between Igbo (57.4%), Bini (52.7%) and other minor tribes in Edo states (52.8%), there was no statistical difference in the prevalence (p = 0.668). This study showed that Christians and Moslems perceived musculoskeletal symptoms with no statistical difference in the prevalence; Moslems (66.7%) and Christians (48.3%) p = 0.275.
Parity had an association with musculoskeletal morbidity. The higher the parity, the higher the prevalence of musculoskeletal problems, as seen in multipara (54.8%) against 36.9% in primipara (p = 0.025). Prevalence of musculoskeletal problems increased with increasing BMI ranging from 13.0% through 37.7% to 49.3% for average weight, overweight and obesity, respectively.
In this study, previous trauma to the musculoskeletal system was noted as the factor that caused the highest (100%) development of musculoskeletal problems in Pregnancy. Other factors that caused a rise in the prevalence were previous delivery of a macrosomic baby (92.3%), previous caesarean section (77.3%) and experience of musculoskeletal morbidity before current Pregnancy with p-values of 0.000 – 0.006.
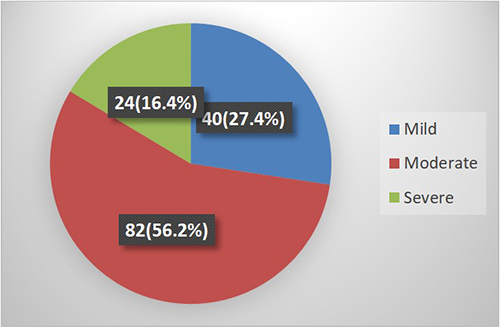
Figure 4: Respondents' perception of the degree of musculoskeletal problems (n=146)
Figure 4: Showed the distribution of Respondents' perception of the degree of musculoskeletal problems. The musculoskeletal symptoms were primarily perceived as moderate 82(56.2%) to severe 24(16.4%) pains.
Table 4: Impact of the musculoskeletal problem on the quality of life of respondents (n=146)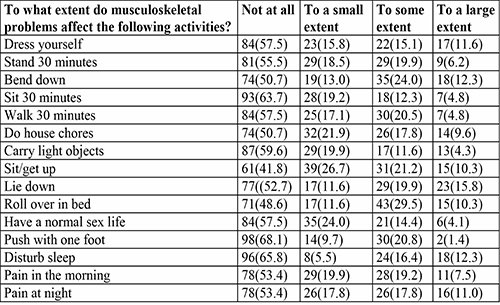
Table 4: Showed the distribution of the impact of musculoskeletal problems on the quality of life of affected respondents. To a large extent, the pain mainly affected respondents' ability to roll over in bed at 39.8%, followed by bending at 36.3% and lying down at 35.7%. Other effects were sleep disturbances 28.7%, inability to do routine household chores 27.4% and difficult sexual life 18.5%. There was no significant diurnal variation in the severity of the pain, 26.7% versus 28.8% for morning and night, respectively.
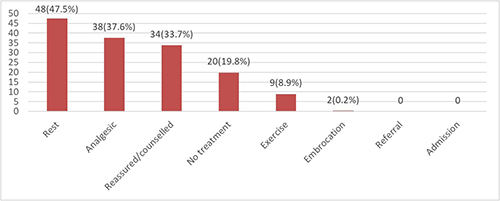
Figure 5: Treatment modalities offered for musculoskeletal problems (n=101)
Figure 5: Showed the distribution of treatment modalities offered to the respondents for their musculoskeletal problems. Though 146 respondents experienced musculoskeletal symptoms in index pregnancy, only 101(69.2%) complained to their physicians, and they mainly were counselled to rest 48(47.5%). Other treatments were oral analgesics 37.6%, reassurance 33.7%, exercise 8.9% and embrocation 0.2%. None were referred to other specialists, and 20(19.8%) had no treatment prescribed for them.
Table 5: Respondents' improvement and satisfaction with treatment offered for musculoskeletal problems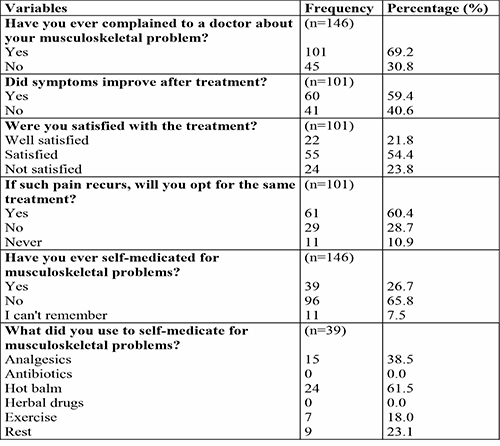
Table 5: Shows the distribution of the respondents' level of improvement and satisfaction with treatment offered for musculoskeletal problems. Out of the 101 that were provided different treatment modalities, more than half 60(59.4%) had their symptoms improved/relieved, most (76.3%) were satisfied with the treatment offered to them, and 61(60.4%) were ready to accept the same treatment if the symptoms recur in their subsequent Pregnancy. Thirty-nine (26.7%) resorted to self-medication using hot balm 24(61.5%), oral analgesics 15(38.5%), rest 9(23.1%) and exercise 7(18.0%). None used antibiotics or herbal concoctions.
Discussion
This study showed the prevalence of musculoskeletal problems, which were essentially pains in Pregnancy, to be 48.7%, with 146 of the 300 pregnant women that responded experiencing some form of musculoskeletal problems. Similar to the findings of (50.7%) by Yasobat et al. in their study in India,8 Ramchandra et al.; anticipated 50% also in India11 and Idowu et al. (53.8%) in their study among women in Benin though not during Pregnancy.12 In their study in Southeast Nigeria, Adinma et al. reported a prevalence of 55.7% which is slightly higher than the value in this study.1 Also, a prevalence of 67% of musculoskeletal problems in Pregnancy was reported in the United States by Clayton et al.10 The high value in the latter may be due to environmental effects, with pregnant women in developed countries having higher perception and response to pains than their counterparts in developing countries like Nigeria and India.8,10
The study also confirmed onset of musculoskeletal problems in Pregnancy is mostly in 3rd trimester, 49.3%, followed by 2nd trimester, 32.2% and at least in 1st trimester, 18.5%. It equally showed higher prevalence with increasing gestational age such that 90 out of 150 (60.0%) in their 3rd trimester had musculoskeletal symptoms; 45 out of 100 (45.0%) in their 2nd trimester experienced it, while only 11 out of 50 (22.0%) in their 1st trimester had the symptoms. Kesikburun et al. observed that musculoskeletal dysfunction usually complicates Pregnancy in the second (17.3%) and third (55.9%) trimesters.2 The higher prevalence with an increase in gestational age is due to a progressive increase in the concentration and effects of the pregnancy hormones and an increase in physical changes associated with Pregnancy as pregnancy advances.1-4
Pelvic pain was the most common (48.8%) musculoskeletal problem experienced by respondents in this study, followed by low back pain 43.2%, with wrist/hand pain being the least 10.3%. None in this study experienced shoulder, neck, or elbow pains. Similar to the result of Adinma et al. in Southeast Nigeria, where they observed that pelvic pain was the commonest problem, though with a higher incidence of 70.3% and Low back pain of 23.4%.1 Kesikburun et al. also observed that wrist/hand pain had the least incidence.2 The higher incidence of pelvic pain can be explained by increased foetal weight and pelvic pressure as pregnancy advances.
Also, it was observed that previous trauma to the musculoskeletal system was the factor that caused the highest (100%) development of musculoskeletal problems in Pregnancy. Other factors that caused a rise in the prevalence were previous delivery of a macrosomic baby (92.3%), previous caesarean section (77.3%) and history of musculoskeletal morbidity prior to current Pregnancy. Luan et al. also made similar findings in their work, noting that women with a previous history of musculoskeletal disorders were more prone to musculoskeletal disorders.6 Corroborated by Previous Studies.1-5 Other notable factors associated with a rise in the prevalence of musculoskeletal symptoms include a higher level of education, as respondents with tertiary level of education perceived the symptoms more (54.4%) than those with secondary (32.3%) and primary (14.3%). Furthermore, higher parity (54.4 % of multipara) and higher body mass index (87.0% of both overweight and obesity) also influence the prevalence. Socio-economic factors like maternal age, tribe, religion and profession did not influence the prevalence of the morbidity. Some other researchers observed the same except that of maternal age.1,18
Most respondents (56.2%) perceived musculoskeletal problems as moderate pain, with 27.4% and 16.4% perceiving them as mild and severe, respectively. Conversely, Meron noted 25% with severe symptoms.9 Together, 72.2% perceive it as moderate to severe pain. Thus, musculoskeletal problems in Pregnancy are not mild pains that healthcare givers can overlook during antenatal.
The pain mainly affected respondents' ability to roll over in bed at 39.8%, followed by bending at 36.3% and lying down at 35.7%. Other effects were sleep disturbances 28.7%, inability to do routine household chores 27.4% and difficult sexual life 18.5%. Similar to the finding by Manyozo et al., where 30% could not do their regular household chores, 34% had difficulty in normal sexual activity, and 43% had sleep disturbances.20 There is no significant difference in the number of respondents who felt the pain more in the morning; 39(26.7%), than at night; 42(28.8%); contrary to the findings of Kesikburun where 57.6% experienced the pain more at night.2 Yasobant, Ayanniyi and co-workers also made the same observation as the latter.8,25
Even though most respondents (72.6%) perceived these musculoskeletal symptoms to be moderate to severe, of the 101(69.2%) that complained to their caregiver, the treatment was majorly rest (47.5%). In comparison, 19.8% had no treatment, and 33.7% were just reassured. Thus, about half of the affected respondents (53.5%) had no treatment, while none were referred to other specialists for a multidisciplinary approach. Similar to the done by Adinma in Southeast Nigeria (46.8%) but at variant with that done by Jimoh in Ilorin-Nigeria where 48.3% were co-managed with physiotherapist.1,36 It is also different from what obtains in the USA where such patients were co-managed or referred to orthopaedic surgeons, physiotherapists or chiropractics.35
Sixty (59.4%) of those treated had their symptoms relieved, and 76.3% were satisfied with the treatment offered, so 60.4% were ready to accept the same treatment modality if the symptoms recur in their subsequent Pregnancy. However, about a quarter (23.8%) was not satisfied with their treatment modalities, for which 26.7% resorted to self-medication though none used herbal concoction. Ayanniyi et al. in Ibadan-Nigeria also observed a 50% resolution of symptoms by postural modification.25 Clayton in the USA also noted that only 10% were satisfied with the symptom relief they obtained after treatment.35 Thus, it calls for collaboration with other relevant disciplines in managing pregnant women with these problems to provide comprehensive health care during Pregnancy.
Conclusion
This study has shown that about half the women who present for antenatal care experience some form of musculoskeletal problem. The commonest predisposing factor was previous musculoskeletal trauma, and pelvic pain was the most common musculoskeletal problem. The symptoms were mainly perceived to be moderate and affected their quality of life. About half of the affected women had no specific treatment, and a quarter were unsatisfied with the treatment offered. Therefore, Clinicians should inquire about musculoskeletal problems in otherwise healthy pregnant women during antenatal care for a multidisciplinary approach to provide comprehensive health care in Pregnancy.
References
- Adinma JIB, Adinma ED, Umeononihu OS, Oguaka V, Adinma-Obiajulu ND, Oyedum SO. Prevalence, Perception and Risk Factors for Musculoskeletal Discomfort among Pregnant Women in Southeast Nigeria. Journal of Musculoskeletal Disorders and Treatment. 2018;4(063): 1-9.
- Kesikburun S, Guzelkucuk U, Fidan U, Demir Y, Egrun A, Tan AK. Musculoskeletal pain and symptoms in Pregnancy: a descriptive study. PMC home journal list Ther Adv Musculoskel Dis. 2018; 10(12): 229-234.
- Sakamoto A and Gamada K. Altered musculoskeletal mechanics and risk factors for postpartum pelvic girdle pain: a literature review. J Phys Ther Sci 2019(10): 831-834.
- Riahi H, Mechri-Rekik M, Bouaziz M, Ladeb M. Pelvic Musculoskeletal disorders related to Pregnancy. J of Belgian Society of Radiology 2017; 101(S2): 2
- Bingefors K, Isacson D. Epidemiology, co-morbidity and impact on health-related quality of life of self-reported headache and musculoskeletal pain- a gender perspective. Eur J pain 2004;8(5): 435-450.
- Luan HD, Hai NT, Xanh PT, Giang HT, Thuc PV, Hong NM, et al. Musculoskeletal Disorders: Prevalence and Associated Factors among District Hospital Nurses in Haiphong, Vietnam. BioMed Research International. 2018; ID 3162564:9
- Borg-stein J, Dugan SA. Musculoskeletal disorders of Pregnancy, delivery and postpartum. Phys. Med Rehabil Clin N AM 2007; 18(3): 450-476.
- Yasobant S, Nibedita S, Arnansu M, Kirti S. Muscuoskeletal Problems among Pregnant Women : A facility based survey in Odisha. Intl J Med Res & Health Sci. 2014;3:2 358-363
- Meron A. Musculoskeletal issues in Pregnancy. http://cusportsmedcenter.com >M
- Clayton D, Skaggs DC, Nelson M. Back and Pelvic Pain in an Underserved United States Pregnant Population: A Preliminary Descriptive Survey. J Manipulative and Physiological Therapeutics. 2007;30(2): 130-134.
- Ramchandra P, Maiya A, Kumar P, Kamath A. Prevalence of musculoskeletal Dysfunctions among Indian Pregnant Women. J Pregnancy 2015:437105.
- Idowu OA, Adeniyi AF, Babatunde OA, Atijosan OJ. Prevalence of self-reported low back pain among patients with type 2 diabetes mellitus: A preliminary survey. East African orthopaedic jour. 2015; 9:9-11.
- Munabi Ig, Buwembo W, Mwaka ES. Musculoskeletal disorder risk factors among nursing professionals in low resource settings: a cross-sectional study in Uganda. BMC Nursing 2014;13:7
- Maduagwu SM, Maijindadi RD, Duniya KI, Oyeyemi AA, Saidu IA, Aremu BJ. Prevalence and Pattern of work–related disorders among Bankers in Maiduguri, Northern Nigeria. Occupational Medicine and Health Affairs. 2014.
- Zaghw A, Koronfel M, Podgorski E, Siddiqui S, Valliani A, Karmakar A, Khan J. Pain Management for Pregnant Women in the Opioid Crisis Era. Intechopen 2018; DOI:10.5772/intechopen.779333.
- Weber SE. The cultural aspect of childbearing women. JOGNN 1996;25:67-72.
- Akadri AA, Odelola OI. Labour pain perception: experiences of Nigerian mothers. Pan Afr Med J 2018;30 288.
- Wang S, Dezinno P, Maranets I, Berman MR, Caldwell-Andrews AA, Kain ZN. Low back pain during Pregnancy: Prevalence, risk factors and outcomes. Obstet Gynecol 2004;104(1): 65-70
- Carvalho ME, Lima LC, Terceiro CA, Silva MN, Cozer GA, Couceiro TC. Low back pain during Pregnancy. Rev Bras Anaestesol.2017;67(3): 266-70.
- Manyozo SD, Nesto T, Bonongwe P, Muula AS. Low back pain during Pregnancy: Prevalence, risk factors and association with daily activities among pregnant women in urban Blantyre, Malawi. Malawi Med J 2019;31 (1): 71-76
- Fariba G, Jafarabadi A, Mohammed, Bandpei M, Ali M. Prevalence of musculoskeletal pain and associated factors with low back pain during Pregnancy. Iranian J of obstetrics, gynae and infertility.2013; 15(41): 9-16.
- Thabah M, Ravindran V. Musculoskeletal problems in Pregnancy. Rheumatology Int. 2014 DOI: 10.1007/s00296-014-3135-7
- Bermas BL Lockwood CJ, Eckler K. Musculoskeletal change and pain during Pregnancy and postpartum. UpToDate, Wolter Kluwer Health. 2017
- Ritchie JR. Orthopaedic Considerations during Pregnancy. Clin Obstet Gynaecol. 2003;46:456-466.
- Ayanniyi O, Sanya AO, Ogunlade SO, Oni-Orisan MO. Prevalence and Pattern of Pain among pregnant women attending Ante-natal Clinic in Selected Health Care Facilities. Afr. J. Biomed. Res 2006;9:149-156.
- Vleeming A, Albert HB, Ostgaard HC, Struresson B, Stuge B. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J 2008;17:794-819.
- Wu WH, Meijer OG, Uegaki K, Mens JMA, van Dieen JH, Wuisman PIJM, et al. Pregnancy-related pelvic girdle pain (PPP), I: terminology, clinical presentation and prevalence. Eur Spine 2004;13;575-580.
- Montella BJ, Nunley JA, Urbaniak JR. Osteonecrosis of the femoral head associated with Pregnancy. A preliminary report. J Bone Joint Surg AM 1999; 81; 790.
- Lose G, Lindholm P. Transient painful osteoporosis of the hi in Pregnancy. Int J Gynaecol Obstet 1986; 24:13.
- Young GL, Jewell D. Interventions for leg cramps in Pregnancy. Cochrane Database Syst Rev CD000121. 2002.
- Foye PM, Patibanda V. Physical medicine and rehabilitation for De Quervain Tenosynovitis. Medscape 2016.
- Choi HJ, Lee JC, Lee YJ, Lee EB, Shim SS, Park JS, et al. Prevalence and clinical features of arthralgia/arthritis in healthy pregnant women. Rheumatol Int 2007; 28 1111-1115.
- Sumilo D, Kurinczuk JJ, Redshaw ME, Gray R. Prevalence and impact of disability in women recently giving birth in the UK. BMC Pregnancy Childbirth 2012; 12:31.
- Liddle SD, Pennick V. Interventions for preventing and treating low back and pelvic pain during Pregnancy. Cochrane Database Syst Rev 2015; Cd001139.
- American Chiropractic Association. Women Need Expanded Musculoskeletal Care During Pregnancy.2007
- Jimoh AAG, Omokanye LO, Salaudeen AG, Saidu R, Saka MJ, Akinwale A, et al. Prevalence of low back pain among pregnant women in Ilorin, Nigeria. Academic journal. 2013; 4(4):23-6.