Gender based violence among pregnant women in Benin City, Edo State: Prevalence, categories, patterns and associated factors
Obi A I1, Adeola V O2, Eriki O J1, Imadojiemu O M1, Adayonfo E2, Obi J N3, Obi R U1
Abstract
Context: Gender based violence (GBV) is a global public health issue common in pregnancy.
Objective: To assess GBV among pregnant women in Benin City with aim of curbing its occurrence.
Study design: A facility based analytical cross-sectional study was conducted involving consenting pregnant women
Results: Awareness of GBV was high 462 (92.4%), with media 293 (63.4%), friends 251 (54.3%) and family members 187 (40.5%) reported as the main sources of information respectively. The overall prevalence of GBV was 288 (62.3%) while in relation to category of GBV experienced; 365 (79.0%), 286 (61.9%), 218 (47.2%) and 216 (46.8%) reported emotional abuse, sexual abuse, physical abuse and economic abuse respectively. Prevalence of GBV was significantly associated with respondent’s level of education (p=0.024) and occupational class (p=0.002). Furthermore, among respondent’s partners smoking (p < 0.001), alcohol consumption (p<0.001), keeping multiple sexual partners (p < 0.001), aggressive traits (p < 0.001), level of education (p < 0.001) and employment status (p=0.005) were significant factors exhibited by them.
Conclusion: Gender based violence was prevalent among pregnant women studied, a comprehensive strategy targeted at sensitizing pregnant women and their partners on GBV will be useful in curtailing its occurrence.
Key words: Antenatal clinic, Awareness, Benin City, Edo State, Gender based violence, pregnant women.
Introduction
Gender – based violence (GBV) is an umbrella term for any harmful threat or act directed at an individual or group based on actual or perceived biologic sex, gender identity and/or expression, sexual orientation, and or lack of adherence to socially constructed norms around masculinities and femininities. It is rooted in structural gender inequalities, patriarchy, and power imbalances.1,2
GBV is violence involving and being perpetuated by men and women, although females are usually the victim derived from unequal power relationships between men and women. Gender based violence remains one of the most rigorous challenges to women’s health and well-being, it is one of the indispensable issues of equity and social justice.3,4 Gender based violence (GBV) is generally understood to include physical (i.e. pushing, kicking, throwing objects, hitting with hands or objects, choking, attacking with a knife or blade), sexual (i.e. forced sexual relations), and psychological (i.e. insults, belittlement, threats, to or threat of abandonment) abuse from intimate partners, sexual violence by non-partners, sexual abuse of girls, and acts such as trafficking women for sex.2,4 Intimate partner violence (IPV) is a very common form of GBV reported against women globally, it is characterized by physical, sexual, or emotional abusive acts as well as controlling behaviours.1,5-8 IPV can occur during pregnancy and the perinatal period, and is increasingly being recognized as an important risk factor for adverse health outcomes for both mother and newborn. Intimate partner violence is widespread in Sub-Saharan Africa; surveys conducted in the region showed that 46% of Ugandan women, 60% of Tanzanian women, 42% of Kenyan women, and 40% of Zambian women reported regular physical abuse.9
According to Centre for Disease Control and Prevention (CDC), pregnancy may represent a unique opportunity for the vulnerable woman to have contact with health care providers, making it an important time for the detection of violence during and after the pregnancy.10 The prevalence rate of intimate partner violence during pregnancy ranges between 4 and 29%.11 Intimate partner violence (IPV) during pregnancy affects the woman’s reproductive health, imposes fatal and non-fatal adverse health outcomes on the growing fetus due to the direct trauma of abuse to a pregnant woman’s body, as well as the physiological effects of stress from current or past abuse on fetal growth and development.1 These events increases likelihood of miscarriage,12 premature labour or delivery,13 low birthweight,14,15 higher levels of depression during and after pregnancy16 and injury.17 Indirect health effects include substance abuse,18 delay in seeking antenatal care,19 insufficient weight gain during pregnancy20 and reduced levels of breastfeeding.21
Although, legislations exist to prevent and address GBV at both international and national levels, these laws are not uniformly enforced. In Nigeria, Violence Against Persons Prohibition (VAPP) Act 2015 recognizes GBV as a form of discrimination and recommends that states take measures to prevent and respond to violence against persons under section 44 of the (VAPP) Act.22
This study was conducted to assess the prevalence, category, patterns and associated factors of GBV among pregnant women towards GBV in Benin City in other to curb this public health problem.
Materials and methods
This study was conducted in Benin City, the capital city of Edo state, Southern Nigeria. Study was carried out in two hospitals (one tertiary, one secondary) that provide Antenatal care services. These hospitals are located in Egor Local Government Area and Oredo Local government area respectively in Edo State.23 English and pidgin English are the commonly spoken, Christianity remains the dominant religion with Islam and African traditional religions also practised in this area.23,24
A Facility based analytical cross-sectional analytical study design was utilised for the study from July 2015 to July 2016. Structured pre-tested structured questionnaires were administered to consenting pregnant women (15-49years) attending antenatal clinics in University of Benin Teaching Hospital (UBTH) and Central Hospital Benin City, Edo State. A minimum sample size of 355 respondents was calculated using Cochran formula25 based on a 36% prevalence of GBV reported in a previous study.26
A systematic random sampling technique was used to select participants from the health facilities selected until the desired sampled size was obtained. A pre-test was carried out and necessary adjustment with modifications made on the study tool prior to actual commencement of data collection. Awareness of GBV was assessed based on those who have heard of the term GBV. Knowledge of GBV was assessed using 39 questions under 7 domains, with a Cronbach’s alpha score of 0.781. A score of 1 was given for every correct response and 0 for an incorrect response, unanswered variables also attracted a score of 0. The total point score was 39, a percentage composite score of greater than or equal to 50% was categorized as good knowledge, while less than 50% was categorized as poor knowledge.
Attitude towards GBV was assessed based on 9 questions scoring system, with a Cronbach’s alpha score of 0.650. A score of 1 was allotted for each appropriate response and 0 for every inappropriate response, giving a total aggregate score of 9. An aggregate score of greater than or equal to 50% was categorised as positive attitude (supportive of GBV) while less than 50% was categorised as negative attitude (not supportive of GBV).
Prevalence of GBV was based on a composite score system involving a total of 4 questions with a Cronbach’s alpha score of 0.779. For every question, a score of zero was given for never experience of GBV while one for ever experience of GBV, giving a total of four-point score. This point score was converted to percentage score, a percentage point score of 1-100 was considered to have experienced GBV while that of zero was considered not have experienced GBV. The occupation of respondents was coded using the skill levels according to ILO classification which was modified for the purpose of this study into skill level 0, 1, 2, 3 and 4
• Skill level 0: house wives, unemployed persons and students
• Skill level 1: performance of simple and routine physical or manual tasks and may require primary or no level of education eg. cleaners, farmers, laborers.
• Skill level 2: occupations requiring high level of manual dexterity and usually a secondary level of education. e.g. Secretary, police officers, hair dressers, tailors and butchers
• Skill level 3: occupations requiring a high level of literacy, numeracy and good communication skills, usually obtained following higher education for a period of 1-3 years e.g. Shop managers, medical radiographers, legal secretaries, medical laboratory technicians
• Skill level 4: occupations typically involving complex problem solving, decision making and creativity based on extensive knowledge in a specialized field. These occupations require a 1st degree or higher qualification eg. Medical practitioners, civil engineers, secondary school, teachers, bankers, accountants and marketing managers.
Data collected were sorted completeness and analysed using SPSS version 20.0 statistical software with statistical significance set at p˂0.050 and 95% Confidence Interval.
Results
The mean age of the respondents was 30.2 ± 4.9 years, Benin 228 (45.6%) and Christianity 478 (95.6%) were the major ethnic group and religion respectively while 470 (94.0%) of the respondents were married. Three hundred and fourteen (62.4%) and 177 (35.4%) of respondents had tertiary level of education and were in skilled level 2 occupational class. Finally, in relation to employment status, majority 308 (79.4%) of respondents were employed while 192 (20.6%) were unemployed.
In relation to level of awareness on Gender based violence, 462 (92.4%) of respondents were aware of the term GBV, with media 293 (63.4%), friends 251 (54.3%) and family members 187 (40.5%) reported as the main sources of information. Furthermore, 252(54.5%) and 210 (45.5%) of respondents studied had poor and good knowledge of GBV respectively. Finally, 334 (72.3%) and 128 (27.7%) had negative and positive attitude towards gender-based violence respectively.
Table 1: Category and prevalence of GBV among pregnant women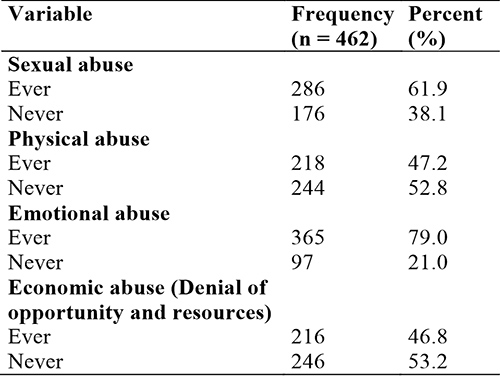
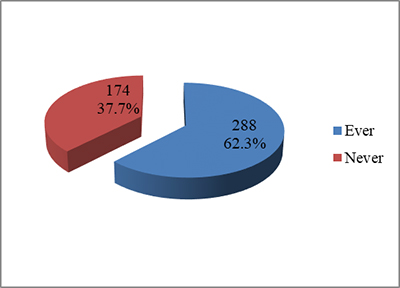
Figure 1: Prevalence of gender based violence among pregnant women in Benin City
In relation to prevalence and categories of GBV among pregnant women studied (See Table 1 above); 365 (79.0%), 286 (61.9%), 218 (47.2%) and 216 (46.8%) of respondents had experienced emotional abuse, sexual abuse, physical abuse, denial of opportunity and resources respectively.
In general, 288 (62.3%) of respondents studied had experienced a form of GBV while 174 (37.7%) had not experienced any form of GBV (See Figure 1)
In relation to the pattern of sexual abuse among respondents (See Table 2); unwanted kisses 218 (47.2%), unwanted fondling or touching of genitals and buttocks 208 (45.0%), forced to do something sexual they found degrading or humiliating 160 (34.6%) and rape 77 (16.7%) were reported by respondents. In relation to perpetrators, 71 (51.4%) attributed to husbands, 12 (8.7%) partners while 1 (0.7%) each by their children and in-law, they were however silent on perpetrators in 51 (36.7%) of victims.
Table 2: Pattern of Sexual abuse among pregnant women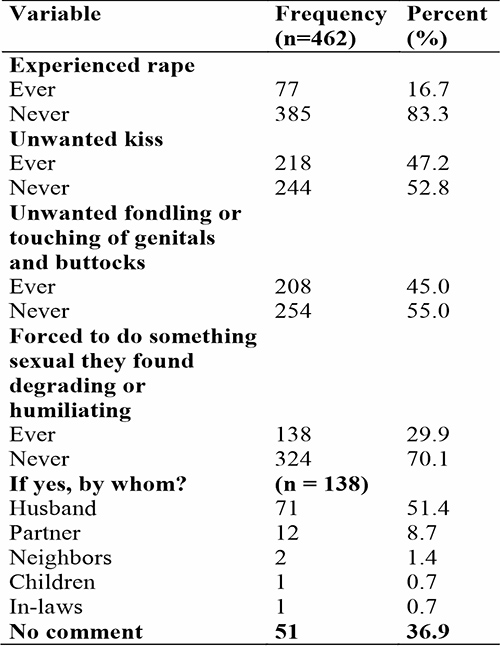
In relation to the pattern of physical abuse among respondents (See Table 3); hits or slaps 166 (35.9%), kicks, punches or shoves 110 (23.8%), being beaten or dragged 102 (22.1%), burnt or choked on purpose 59 (12.8%) and use of any weapon against you 83 (18.0%) were reported by respondents. In relation to perpetrators, over half of them were abuse by husband 37 (44.6%) and partners 12 (8.7%) while 1 (0.7%) by their children, furthermore 51 (36.7%) of them were silent on the perpetrators.
Table 3: Pattern of physical abuse among pregnant women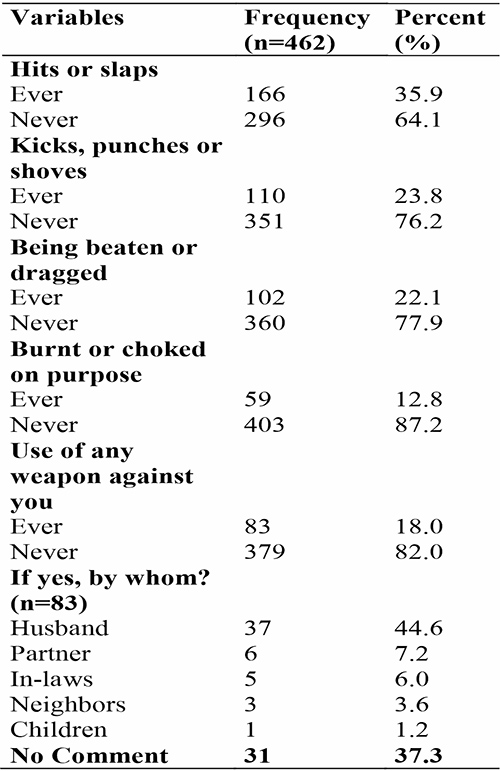
In relation to the pattern of emotional abuse among respondents (See Table 4); wanting to know your whereabouts at all times 323 (69.9%), verbal insults in public or private 286 (61.9%), ignoring and treating you indifferently 223 (48.3%) and forced isolation from friends 182 (39.4%) In relation to perpetrators, less than two-third of them were emotionally abuse by husband 112 (50.2%) and partners 27 (10.3%) respectively, the least was by neighbors 4 (1.8%). Furthermore 69 (30.9%) of them were silent on the perpetrators. In relation to the prevalence of economic abuse (See Table 5); 216 (46.8%) had experienced denial of opportunity and resources while 246 (53.2%) had not.
Table 4: Pattern of emotional abuse among pregnant women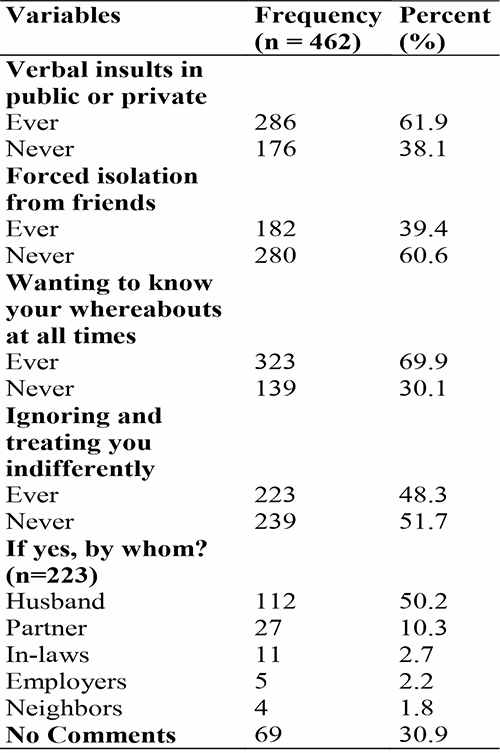
Table 5: Prevalence of economic abuse among pregnant women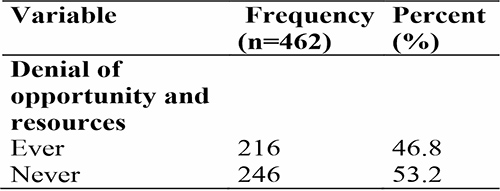
In relation to factors associated with GBV among pregnant women (See Table 6), Educational status (p=0.024) and occupational class (p=0.002) were identified as significant factors. Furthermore, employment status (p=0.249), Religion (p=0.535), Parity (p=0.156), Marital Status (p=0.088) and Age group (p=0.417) were not identified as significant factors influencing GBV among pregnant women.
Table 6: Factors associated with GBV among respondents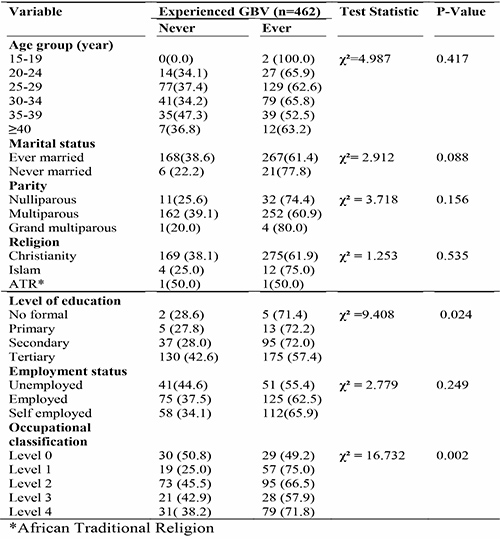
In relation to factors influencing GBV by partners of pregnant women (See Table 7), smoking (p<0.001), drinking alcohol (p<0.001), victim of abuse (p=0.003), being aggressive (p<0.001), having multiple sex partners (p<0.001), level of education (p<0.001), employment status (p=0.005) were identified as significant factors. Finally, being the bread winner (p=0.270) and coming back late (p=0.430) were not identified as significant factors influencing GBV by partners of pregnant women in Benin City, Edo State.
Table 7: Factors influencing perpetuation of gender based violence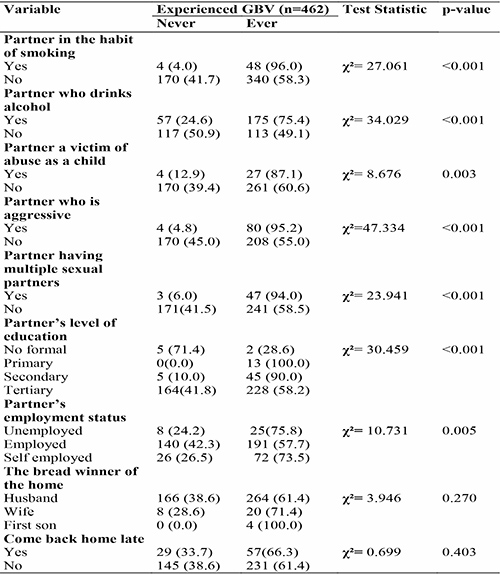
Discussion
About two-third of respondents fell within the 25-34 age group category, this is consistent with the reproductive age group, this findings is similar to those from previous studies carried out in Zaria27 and Enugu.28 Meanwhile, women who were in the teenage age range 15-19 years formed the least proportion of <1%. This may be attributed to the fact that there’s an increasing awareness of the benefit of female education to health, wellbeing and socio-economic growth of the society, thus more women tend to delay childbearing till a later age. In addition, all the respondents studied fell into the reproductive age group (15-49 years).
Most of our respondents were Benin, which is the predominant tribe in the study area. Majority of the respondents studied practiced Christianity, which is in keeping with 2018 NDHS report which found that Christianity is the dominant religion in southern Nigeria.29
Almost all of the respondents had been married and this may be due to the cultural stigma which comes with pregnancy while unmarried. The Nigerian society perceives pregnancy in an unmarried woman as an impression of promiscuity, hence women would prefer to begin child bearing only after marriage. Meanwhile, women who eventually get pregnant out of wedlock resort to a secretive lifestyle and may not want to seek public attention in the form of antenatal care, this in itself may have far reaching health and socio-economic implications.
An estimated four-fifth of our respondents were multipara, this is similar to findings from a study done in Zambia,30 this finding is a reflection of the high fertility rate and possibly low contraceptive uptake among study population within the study area and by extension Nigeria.29
Majority of the antenatal attendees had completed secondary or tertiary education; this is in tandem with findings from a study conducted in Lagos Nigeria.31 This may be explained by the fact that women with higher level of education are more enlightened about the possible risks of pregnancy and thus more likely to seek antenatal services from a health facility. This also highlights the fact that as opposed to the past when women were viewed as being confined to the kitchen, there’s more enlightenment on the importance of female education. Majority of respondents studied were employed, having some means of livelihood and by implication economic relevance in terms of what they can bring to the table.
Awareness of gender-based violence was high among study population and this finding is similar to studies done in Zaria27 and Abuja32 with media being the main source of information. This may be due to the high level of education among respondents. This is commendable and if well harnessed could evolve into behavioural changes over time contributing to curbing the GBV scourge.
Despite the high level of awareness of GBV, majority of respondents had poor knowledge of GBV and may be because the respondents did not know what constitutes GBV as only 35.5% and 33.2% identified correctly the place of occurrence of GBV, perpetrators of GBV, its consequences and policies in place to combat this menace. This is emphasized more by the fact that a higher proportion of respondents heard from media, friends or family members; these sources may provide only superficial information on the subject matter thus restricting the level of knowledge of these respondents. Furthermore, the school as a place where people are likely to gain in depth knowledge of a topic, accounted for the least proportion (19.6%). This is of concern as what is not clearly known cannot be consciously prevented, and this calls for increased in-depth enlightenment of the public on what constitutes GBV through verifiable sources such as schools and even health care personnel/providers during routine ANC clinic visits.
Also, poor knowledge of GBV could form a vicious cycle perpetuating GBV because victims and perpetrators may find it difficult to prevent what they may not recognize as acts of GBV. This in itself could influence reporting of GBV and thus implication and impact for health, wellbeing and socio-economic development.
In this study, knowledge of GBV was found to increase with increasing level of education. This is in line with studies conducted in Enugu28 and justify the need for education of females early especially as girl child. Education tends to increase mental capacity and thus increase the ability and chances to access information both from the media and other sources like books, magazines etc.
Poor knowledge of GBV was more with increasing parity and among the ever-married respondents. This may be that these respondents are more likely to be older and thus may not have benefitted from the new trend of better female education. These respondents may also be more likely to agree with the socio-cultural view of GBV as a normal aspect of life. This buttresses this study’s finding of a higher proportion of respondents with good knowledge among the younger age groups (20-29 years) as opposed to a higher proportion of respondents with poor knowledge among the older age groups (30-44 years). This draws attention to the fact that with emerging campaigns; the younger generation seems to abhor the act of GBV to a greater extent, also could be more proactive and vocal against issues of abuse.
In this study, over three quarters of respondents had negative attitude towards GBV and are thus not supportive of GBV. This finding is in contrast with studies done in Zaria27 and Delta,33 where majority of respondents were indifferent or condoned the act. This finding may be attributed to the fact that majority of the women in our study had tertiary level of education which may inform decisions and reduce the likelihood of complete economic dependence on spouse. This is further strengthened by the increasing negative attitude towards GBV with increasing level of education of respondents also identified in this study.
It is of concern that despite the adverse consequences of GBV among pregnant women.11-21 over four fifth of respondents either agreed or were indifferent about the fact that GBV is a private matter and should be settled without interference. This brings into context the socio-cultural dimension to GBV which a qualitative research would better explore. However, other plausible reasons may include: fear of ridicule from friends and family; economic dependence and the fact that it is seen as failure on the part of the woman for her family matter to be discussed in public.
In this study, a higher proportion of the respondents who had ever been married had negative attitude towards GBV. This may be explained in part as these respondents may more likely have experienced GBV and are more abreast with possible consequences and hence, less likely to support GBV. In the same vein, majority of the respondents studied who had good knowledge also had negative attitude towards GBV. In contrast, positive attitude towards GBV was more among grand-multipara than others, this was further corroborated by the higher prevalence of GBV observed among this category of respondents. These respondents may be more likely to be tolerant in an abusive relationship based on the mind-set that they have more to lose in terms of societal stigma and care of the children in addition to societal acculturation of silence in the midst of issues of concern especially among older respondents.
Despite the high awareness and negative attitude towards GBV, over four-fifth of respondents had experienced one form of GBV or the other. This is in contrast to findings from a study conducted in Jos, Plateau state34 where only 28.9% had been violated in previous pregnancy while 31.8% were violated in index pregnancy. The finding in our study may be due to poor knowledge of the consequences of GBV and policies in place to combat it among our respondents, combined with poor perception of the role of the legal system, this may increase the likelihood for under reporting and thus, encourage perpetrators to continue the act without penalty.
Just above two-third of respondents had experienced sexual abuse, mostly perpetrators by male spouse/partners. This is contrast with a study carried out in Zaria,27 where 22% of the respondents reported experience of sexual abuse. Sexual violence is a serious public health problem and it has both short and long–term negative physical and psychological effects on health and well-being such as miscarriage, still birth, preterm birth, foetal injury and low birth weight, increased mental health problems, suicide attempts, worsening of chronic illness, injury, substance abuse and gynaecological problems.11-21 Furthermore, findings from our study revealed that just below half of our respondents were physically abused, this is contrast to findings among pregnant women attending ante natal clinic in Nsanja District, Malawi.35
Emotional abuse had been experienced by over three-quarter of respondents. This is in contrast with studies carried out among pregnant women attending antenatal clinics in Malawi35 and Abuja, Nigeria32 where 28.1% and 38.0% and were emotionally abused respectively. Emotional abuse has long term debilitating effect on person’s sense of self-esteem and integrity. Often, research has shown that emotional abuse is a precursor to physical abuse.
Results from this study also revealed that a little less than half of our respondents had been denied opportunities and resources. This is in contrast with findings from the study carried out in Abuja,32 where the prevalence was 12.4%.
The more prevalent forms of violence identified in this study were emotional and sexual abuse as opposed to economic and physical abuse. This may be because emotional and sexual abuse are usually perceived by respondents as subtle forms of violence and thus, not seem to necessitate retaliatory actions-such as reporting to appropriate authorities, geared towards eliminating these forms GBV. On the other hand, signs of physical and economic violence are glaring hence the tendency to report such.
Alcohol consumption was identified by majority of respondents to be one of the predisposing factors among partners of respondents who had experienced GBV. This is in line with a study done among pregnant women in Abuja, Nigeria.32 This owing to the fact that alcohol tends to cloud judgement and ability to make sane decisions, thus increasing violent behaviour. Alcohol also reduces the likelihood of amicable settling of misunderstanding among individuals. The injuries sustained from such violence may be fatal or in the long run increase health care cost and lost work time due to more hospital visits, more operational surgeries, and visits to pharmacies.
Findings from this study revealed that a greater proportion of respondent whose partners were smokers had ever experienced GBV, revealing a significant association between a habit of smoking in partner and practice of GBV; this is in line with a study carried out in Plateau state, Nigeria in 2012.34 This may be because smoking and alcoholism are complementary behaviours i.e. those who smoke are more likely to also be alcoholics and thus more likely to exhibit aggressive behaviour thus perpetrate GBV,36 corroborated by the fact that a vast majority of respondents in our study, whose partners were aggressive had ever experienced GBV.
Pregnant non-smokers who live with smokers are more likely to have babies with health problems including prematurity, sudden infant death syndrome (SIDS), impact on the child’s attention, behaviour, and ability to reason and understand thus increasing overall health costs.36,37
Majority of respondents whose partners had Multiple Sexual Partners (MSPs) experienced GBV. This may be because, acquisition of more partners may result in divided attention and resources thus sparking a tendency to treating wife (or primary partner) with disdain and eventually trigger GBV. Furthermore, having MSPs has also been linked with other vices like alcoholism and cigarette smoking which as explained previously, increase the tendency for violent behaviours.
The major bread winner in the home was found to be the husband and this was observed to be a promoting factor for experiencing GBV. Economic violence is more likely to flourish in this setting in the forms of withholding necessities including: shelter, food, clothing, access to money. This forces dependence on the perpetrator financially and diminishes the victim’s capacity for self-support; this will in turn greatly limit the victim’s ability to leave the abusive relationship despite the health and socioeconomic implications.
Furthermore, it was identified in this study that respondents with increasing skill level (i.e skill level 4) were found to have least experienced GBV, thus the higher skill level is a protective factor against GBV. This may be attributable to better economic independence among this category of respondents who may be less likely to be trampled upon by their partner and thus less likely to tolerate an abusive relationship. It is therefore, important to encourage the education of the girl child and woman in addition to exploring all avenues to economically engage and empower them; this would to a large extent help in addressing the scourge of GBV.
Conclusion
Gender based violence was prevalent among pregnant women in Benin City, Edo State. Emotional and sexual abuse were the most common category of GBV identified. There is need for a comprehensive strategy targeted at sensitizing pregnant women and their partners on GBV and implications during and outside the routine antenatal clinics visits to help mitigate GBV and effects among the target population.
Limitations of study
Self-reporting and recall bias could have influenced the results; however, time lines were introduced to help minimize recall bias.
Funding
Research was fully sponsored by authors
Conflict of interest
We hereby declare that the study and manuscript submitted for publication is free of any form on interest and was fully funded by the Authors.
Acknowledgements
We sincerely appreciate the management of University of Benin Teaching Hospital and Central Hospital Benin City for permission and approval to conduct the study. We also appreciate all our research assistants and the respondents that participated in this study.
References
- Berhanie E, Gebregziabher D, Berihu H, Gerezgiher A and Kidane G. Intimate partner violence during pregnancy and adverse birth outcomes: a case-control study. Reproductive health (2019) 16:22. Available from: http://doi.org/10.1186/s12978-019-0670-4.
- United States Agency for International Development (USAID). Gender – based violence. 2016. Available from: https://globalhealthlearning.org/taxonomy/term/878.
- Gurung S and Acharya J. Gender-based Violence Among Pregnant Women of Syangja District, Nepal. Cross Mark and Korea Centers for Disease Control and Prevention. 2016; 7(2), 101-107.
- Pisoh DW, Moses S, Akumawah BZ, Sama DJ, Atabon AF and Foumane P. Gender – Based Violence among Pregnant Women Consulting at the Antenatal Care Unit of the Bamenda Regional Hospital. Open Journal of Obstetrics and Gynecology. 2020; 10(11), 1525-1543. Doi: 10.4236/ojog.2020.10110138.
- C García-Moreno, HA Jansen, M Ellsberg. WHO Multi-Country Study on Women's Health and Domestic Violence against Women: initial results on prevalence, health outcomes and women's responses. 2005; World Health Organization: Geneva.
- S Kishor, K Johnson. Profiling domestic violence: a multi-country study. 2004; ORC Macro: Calverton MD. [Google Scholar]
- R Jewkes. Intimate partner violence: causes and prevention. Lancet. 359(9315): 2002; 1423–1429. [Crossref], [Web of Science ®], [Google Scholar]
- H Johnson, N Ollus, S Nevala. Violence against Women: An International Perspective. 2007; Springer: New York. [Google Scholar]
- CY. Conveying concerns. Women report on Gender – based violence. Women’s edition project. Upper Marlboro: McArdle printing company; 2000.
- Donovan BM, Spracklen CN, Schweizer ML, Ryckman KK and AF Saftlas. Intimate partner violence during pregnancy and the risk for adverse infant outcomes; a systematic review and meta-analysis. BJOG.2016;123: 1289-99.
- Campbell JG-MC and Sharps P. Abuse during pregnancy in industrialized and developing countries. Violence against women. 2004; 10: 770-89.
- AJ Taft, LF Watson. Termination of pregnancy: associations with partner violence and other factors in a national cohort of young Australian women. Australian and New Zealand Journal of Public Health. 31(2): 2007; 135–142.
- T Rodrigues, L Rocha, H Barros. Physical abuse during pregnancy and preterm delivery. American Journal of Obstetrics and Gynecology. 198(2): 2008; 171-6
- E Valladares, M Ellsberg, R Pena. Physical partner abuse during pregnancy: a risk factor for low birth weight in Nicaragua. Obstetrics and Gynecology. 100(4): 2002; 700–705. [Web of Science ®], [Google Scholar]
- CC Murphy, B Schei, TL Myhr. Abuse: a risk factor for low birth weight? A systematic review and meta-analysis. Canadian Medical Association Journal. 164(11): 2001; 1567–1572. [Web of Science ®], [Google Scholar]
- SL Martin, Y Li, C Casanueva, A Harris-Britt. Intimate partner violence and women's depression before and during pregnancy. Violence against Women. 12(3): 2006; 221-9
- D El Kady, WM Gilbert, G Xing. Maternal and neonatal outcomes of assaults during pregnancy. Obstetrics and Gynecology. 105(2): 2005; 357–363.
- MA Curry. The interrelationships between abuse, substance use, and psychosocial stress during pregnancy. Journal of Obstetric, Gynecologic, and Neonatal Nursing. 27(6): 1998; 692–699. [Crossref], [Google Scholar]
- PM Dietz, JA Gazmararian, MM Goodwin. Delayed entry into prenatal care: effect of physical violence. Obstetrics and Gynecology. 90(2): 1997; 221–224. [Crossref],
- CL Moraes, AR Amorim, ME Reichenheim. Gestational weight gain differentials in the presence of intimate partner violence. International Journal of Gynecology and Obstetrics. 95(3): 2006; 254–260. [Crossref], [Web of Science ®], [Google Scholar]
- Y Lau, KS Chan. Influence of intimate partner violence during pregnancy and early postpartum depressive symptoms on breastfeeding among Chinese women in Hong Kong. Journal of Midwifery and Women's Health. 52(2): 2007; 15–20.
- National Agency for the Prohibition of Trafficking in Persons (NAPTIP). Violence against persons (Prohibition) VAPP department. 2021.
- Edo State Statistical Yearbook 2013 Benin City, Nigeria. Edo State Statistical Yearbook 2013 Benin City, Nigeria
- National Population Commission (NPC) [Nigeria] and ICF International. 2014.
- Cochran WG. Sampling Techniques. Third Edition. New York: John Wiley & Sons, Inc.1977:149-156
- Awusi, VO, Okeleke, VO, & Ayanwu, BE. Prevalence of domestic violence during pregnancy in Oleh, a sub-urban Isoko Community, Delta State, Nigeria. Benin Journal of Postgraduate Medicine.2009, 11(1):15-20
- Ameh N and Abdul M. Prevalence of domestic violence amongst pregnant women in Zaria, Nigeria. Annals of African Medicine. 2004; 3(1): 4-6.
- Ezechi OC, Kalu BK, Ezechi LO, Nwokoro CA, Ndububa VI, Okeke GC. Prevalence and pattern of domestic violence against pregnant Nigerian women. J Obstet Gynaecol. 2004 Sep;24(6):652-6. doi: 10.1080/01443610400007901. PMID: 16147605.
- National Population Commission. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, 2019, USA: NPC and ICF.
- Pisoh, D. , Moses, S. , Akumawah, B. , Sama, D., Atabon, A. and Foumane, P. (2020) Gender-Based Violence among Pregnant Women Consulting at the Antenatal Care Unit of the Bamenda Regional Hospital. Open Journal of Obstetrics and Gynecology, 10, 1525-1543. doi: 10.4236/ojog.2020.10110138.
- Adegbite O. and Ajuwon A. Intimate partner violence among women of child bearing age in Alimosho LGA of Lagos State, Nigeria. African Journal Biomed res. 2015;18 (2): 3-17
- Arulogun O. and Jidda K. Experiences of Violence pregnant women attending ante-natal clinics in selected hospitals in Abuja, Nigeria. Sierra journal of biomedical research,2011; 3 (1) 43-48
- Awusi, V, Okeleke V and Ayanwu B. Prevalence of domestic violence during pregnancy in Oleh, a suburban isoko community, delta state, Nigeria, 2009; 11 1-6
- Envuladu EA, Chia L, Banwat ME, Lar LA, Agbo HA and Zoakah AI. Domestic violence among pregnant women attending antenatal clinic in a PHC facility in Jos north LGA Plateau State Nigeria. Journal of medical research, 2012;1(5):63-68
- Robert C, Angela C, Alfred M and Jon O. Magnitude of domestic violence against pregnant women in Malawi. Journal of research in Nursing and midwifery. 2012;1(2):17-21
- Brecklin L. The role of perpetrators alcohol use in the injury outcomes of intimate assault. Journal of family violence, 2012; 17: 185-197.
- West A.,Robert O.,Shiffman S. and Saul L. Fast facts: smoking cessation. Health problems,2007;28-29.