Arrow shot injury to the oro facial regions: Report of two cases
Lawal S H1, Rasheed M W2, Adekunle A A3, Idowu N A4
Abstract
Background: Arrow injury is a case of foreign body impaction. It can affect any part of the body. Arrow injury to the head and neck region can be life-threatening. An arrow is a weapon consisting of a thin, straight stick with a sharp point, designed to be shot from a bow. It is one of the oldest tools for hunt and war. Many health practitioners especially in the developed world now regard arrows as extinct. It has been completely replaced by advanced modern weaponry. This is not the case in our environment where the use of arrows with their attendant injury is still relatively common.
Case report: The first case is a 25-year-old farmer, a Nigerian man was seen at the Accident and emergency unit of our centre with an hour history of arrow injury to the right side of the face following the farmer-herder clash. The examination was remarkable for an impacted arrow that was made up iron (impregenation with poisonous substance could not be ascertained) on the right side of the face. He had an urgent plain radiograph of the head and neck which revealed an impacted arrow in the right zygomatic bone. He subsequently had emergency exploration and removal of the arrow. The post-operative period was uneventful.
The second case was a 37-year-old man who presented to the accident and emergency department with difficulty breathing following an arrow shot injury to the oral cavity. He was a passenger in a bus that was attacked by armed bandits. On examination, there was an arrow penetrating through the right edge of the tongue, the floor of the mouth to the contralateral submandibular and cervical regions. About 5.0cm of the tail of the arrow could be seen jutting out of the mouth. The exploration was done via a Risdon incision (submandibular incision) on the opposite side of the entry wound (left submandibular) in a retrograde approach. The dissection was advanced into the subcutaneous tissue, platysma, and deep fascial plane to expose the tip of the arrow. The post-operative period was uneventful.
Conclusion: We have illustrated our experience on the cases of arrow injury to the orofacial region. The two cases presented early. There was no pre-hospital attempt at pulling out the arrow. Arrow injury is still common in our community. There is a need for government at all levels to intensify effort on conflict management and resolution.
Keywords: Orofacial, Arrow injuries, Face.
Introduction
Arrow injuries to any part of the body parts are a common phenomenon in the North-Eastern part of Nigeria.1 The injuries can involve any part of the body but the most common region of the body are the head and neck, and trunk.2 Arrows with a bow are one of the oldest tools used in war and hunting.3 It is no longer common in the developed world as it has been completely replaced with advanced modern weaponry.4 It is not surprising that injury due to arrow instruments is seen very rarely in the developed world unlike in developing countries. Bow and arrow are in different forms. The severity of injury following a shot arrow is dependent on the type, the velocity at which it is shot as well as the part of the body that is involved. According to Bill, an arrow causes a wound that is both punctured and incised.5 It has an entry point and may have an exit point depending on the level of penetration. Arrow injury to the head and neck region can be devastating and life-threatening. Arrow injury was usually a product of war, hunting, and less commonly archery. In the developed countries of the world, the use of bow and arrow in wars has been replaced by advanced firearms thus significantly reducing the attendant arrow injury to few cases resulting from archery. This is unlike in our community where the use of bow and arrow is still common. The injury is most often the sequel to conflict between nomadic herdsmen and farmers.6 The limitation in availability of grazing land for the normadic herdsmen, scarcity of water and ambulatory nature makes their cows, sheep, and other animals vulnerable to eating up farm plantations which may ignite fracas that might result in a myriad of injuries and death.7 The management of a patient with arrow injury follows the same principles involved in the management of trauma which entails primary survey and resuscitation, secondary survey, ancillary investigation, reevaluation, and definitive treatment.8 Patient is adequately optimized before diagnostic investigation. The diagnosis is confirmed with computed axial tomography following an initial plain X-ray radiograph.9 The treatment is always an emergency exploration for the dis-impaction of the arrow. There is a need for colleagues in various disciplines to be aware of such injuries because managing these patients requires a multidisciplinary approach such as the maxillofacial surgeon, ophthalmologist, otorhinolaryngologist, and neurosurgeon. The government through relevant authorities should be made to understand the consequency of farmers-herders clash which include significant loss of lives, huge economic loss to the nation, and increase in the number of dependants because the majority of people involved are within the working-age bracket. However, a few of them are children below the age of 18.10
Case presentation 1

Figure 1a: Show arrow injury on the right part of the face with the trickling of blood for the first case presentation. 1b: Figure showing the injury on the right orofacial region of the second caseas indicated by the arrow.
A 25-year-old Nigerian man, who presented at the Accident and Emergency unit of our center with an hour history of arrow injury to the right side of the face. The patient was healthy until this unfortunate day while working on his father's farmland observed that herdsmen had allowed their castles to eat up part of the farm composed of grains. The patient tried to reprimand them but this resulted in conflict and arrows were shot. He had a history of pain in the right side of the face. His past medical and surgical history was not remarkable. On examination, the upper and lower third of the face appear clinically normal. there was an impacted arrow on the right middle third of the face located on the lower border of the zygomatic bone with minimal bleeding, swelling and tenderness (Figure1a). Intra-orally, there was a slight limitation of the mouth opening to about 3.0cm of intranasal distance. The tongue, palate, gingiva, buccal mucosa, and floor of the mouth appear clinically normal. A part of the arrow was palpated in the deep upper buccal sulcus.
![]()
Figure 2. Plain radiograph of the skull showing the impacted arrow for the first case presentation.
Urgent X-ray of the head revealed an arrow injury involving the right zygomatic bone with a minor soft tissue injury (Figure2). Complete blood count, serum electrolyte, urea and creatine, and other investigations were essentially normal.
Analgesics, antibiotics, tetanus prophylaxis and intravenous fluid were administered to the patient. He also underwent emergency right facial wound exploration. The surgical technique of the procedure was as follows: following nasotracheal intubation, routine scrubbing, draping, wound exploration and arrow extraction were approached via the wound site anterograde and intraoral buccal sulcus together with a retrograde approach. The arrow penetrated about 6.0cm into the zygomatic bone and the arrow was noticed to have bent due to the thickness of the zygomatic bone. the. The arrow was removed with both anterograde and retrograde approaches by clipping on the bar of the arrow to prevent injury to the vital structures. Another incision was made in the buccal sulcus which was about 4.0cm long, dissected to expose the arrow tip and the arrow was extracted intra-orally to avoid injury to the adjoining soft tissue from the barbs of the arrow. The arrow was successfully removed (figure3a) Immediate and late postoperative periods were not remarkable. The patient was discharged satisfactorily. Follow-up is uneventful.
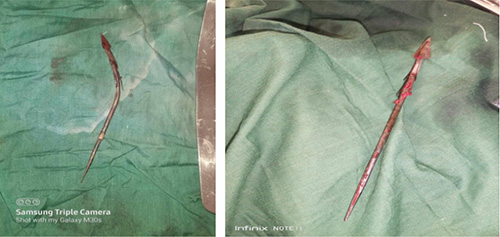
Figure 3. The arrow that were removed for the first(a) case and (b) second case
![]()
Figure 4: The tip of the arrow shot to the oral cavity during intraoperative exploration of the second case
Case presentation 2
A 37-year-old man presented to the accident and emergency department with difficulty breathing following an arrow shot injury to the oral cavity. He was a passenger in a bus that was attacked by armed bandit. Examination revealed a stable patient who is slightly tachypneic with a respiratory rate of 28 cycles per minute, Packed cell volume was 11.0g/dl and other investigations were essentially normal. The upper and middle third of the face appear clinically normal. On the lower third, there was an arrow penetrating through the right edge of the tongue, the floor of the mouth to the contralateral submandibular and cervical regions. (Figure1b) About 5.0cm of the tail of the arrow could be seen jutting out of the mouth. The plain radiograph shows that the tip of arrow was lodged in the left submandibular space. The surgical technique, nasotracheal intubation was not possible in this case, therefore an elective tracheostomy was done. The exploration was done via a Risdon incision (submandibular incision) on the opposite side of the entry wound (left submandibular) in a retrograde approach. The dissection was advanced into the subcutaneous tissue, platysma, and deep fascial plane to expose the tip of the arrow.(Figure 4) The arrow was dissected clear off the soft tissue and extracted via the incision, cleaning the exposed tail with an antiseptic agent to prevent inoculation of infection. The retrograde technique was deployed to remove the arrow and prevent injury to the adjacent soft tissues. The arrow removed as shown in (figure 3b) The wound closure was done in layers using vicryl for deep fascial and prolene for the skin. A drain was applied to prevent hematoma. The immediate post-operation was uneventful and the tracheostomy tube was removed the first postoperative day.
Ethical issues
This case report was conducted in compliance with the guidelines of the Helsinki declaration on biomedical research in human subjects. Consents were obtained from the patients involved in the two cases
Discussion
The management of arrow injury to the head and neck region is challenging.11 Although it is no longer common in most developed and developing countries of the world however it is still a problem in our community. It usually results from farmers-herders clashes most often than not as a result of the invasion of farmlands by nomadic herdsmen with their cattle as reported in some series.12 These cases were similar to the review of orofacial injuries at Federal Medical Centre Nguru where retrospective cases were examined. Notably, the majority of patients were within the age bracket of 10 -70 years, and almost all were males but the circumstances surrounding the arrow shot injuries varied widely. A large proportion of the reported cases were sequel to farmers and herders misunderstanding while a few cases were due to armed bandits. Our case was not an exception. In these cases, the face is the site of the injury and the demographic features of the patients were similar to other reported case series.12,13 This has been said to be the most common part of the head and neck region that may be involved. Not only this but also, this might be related to how the arrow is designed to be shot. The arrows and bow are usually held up high and shot which most often landed in the head while a few of the reports showed chest and abdomen.14 There was not an attempt at forcefully removing the arrow before presentation as reported in some series. This may not be unconnected with the ongoing effort by the health care providers in public enlightenment campaigns on initial trauma care. The diagnosis and extent of the injury were established following a plain radiograph of the head and neck. A computed tomographical scan is said to be the gold standard investigation. It was actually not done in our patient as the information from the plain radiograph was sufficient for surgical intervention and logistics of considerable distance to have CT Scan done. The patient had wound exploration via the entry point for the first case presentation while the contralateral approach was used for the second case via Risdon incision (submandibular incision). We were not unaware of the possibility of approaching the wound via the exit point dependent on the length of the impacted instrument and the surrounding structures however our patient only had an entry wound. The patient did well following the dis-impaction because of prompt presentation and timely intervention by the surgeons and other supporting staff. Furthermore, there were no vital structures or blood vessel involvement.
Conclusion
We have illustrated our experience on the cases of arrow injury to the orofacial region. The two cases presented early. There was no pre-hospital attempt at pulling out the arrow hence reduce morbidity. Arrow injury is still common in our community. There is a need for government at all levels to intensify effort on conflict management and resolution. The immediate mechanism of conflict resolution should be provided at the regional levels by engaging the people's concerns and long-term solutions should be put into place to mitigate the avoidable loss of lives and improve the economy in the region and Nigeria.
References
- Abdullahi H, Adamu A, Hasheem MG. Penetrating arrow injuries of the head-and-neck region: case series and review of the literature. Nigerian Medical Journal: Journal of the Nigeria Medical Association. 2020;61(5):276.
- Jacob OJ, Rosenfeld JV, Taylor RH, Watters DA. Late complications of arrow and spear wounds to the head and neck. Journal of Trauma and Acute Care Surgery. 1999;47(4):768.
- Ramsey S. Tools of War: History of Weapons in Ancient Times: Vij Books India Pvt Ltd; 2016.
- Aremu SK, Dike B. Penetrated arrow shot injury in the anterior neck. International Journal of Biomedical Science: IJBS. 2011;7(1):77.
- Bill JH. ART. II.--Notes on Arrow Wounds. The American Journal of the Medical Sciences (1827-1924). 1862(88):365.
- Ali N, Gali B. Pattern and management of chest injuries in Maiduguri, Nigeria. 2004.
- Idowu AO. Urban violence dimension in Nigeria: Farmers and herders onslaught. Agathos. 2017;8(1):187.
- Jayaraman S, Sethi D, Chinnock P, Wong R. Advanced trauma life support training for hospital staff. Cochrane Database of Systematic Reviews. 2014(8).
- Gracias VH, Reilly PM, Philpott J, Klein WP, Lee SY, Singer M, et al. Computed tomography in the evaluation of penetrating neck trauma: a preliminary study. Archives of Surgery. 2001;136(11):1231-5.
- Wabada S, Abubakar AM, Chinda JY, Adamu S, Bwala KJ. Penetrating abdominal injuries in children: a study of 33 cases. Annals of pediatric surgery. 2018;14(1):8-12.
- Brody JM, Leighton DB, Murphy BL, Abbott GF, Vaccaro JP, Jagminas L, et al. CT of blunt trauma bowel and mesenteric injury: typical findings and pitfalls in diagnosis. Radiographics. 2000;20(6):1525-36.
- Owobu T, Omeje UK, Agbebi SE, Umar AA-h, Tochukwu OB, Bardi M, et al. Management of orofacial arrow injuries at Nigerian tertiary health care hospital: A report of 30 cases. Ibom Medical Journal. 2022;15(1):76-82.
- Adeyemo WL, Ladeinde AL, Ogunlewe MO, James O. Trends and characteristics of oral and maxillofacial injuries in Nigeria: a review of the literature. Head & Face Medicine. 2005;1(1):1-9.
- De S,Dey RS,Biswas SA. Penetrating thorocoabdominal injury with arrow injury:a case report. Int Surg J. 2022;9:734-6.