Congenital pseudoarthrosis of the clavicle co-existing with tetralogy of Fallot: Another variant of the Holt-Oram syndrome?
Essien UE, Dim EM, Nottidge TE, Ubaha AG, Inyang UC
Abstract
Congenital pseudoarthrosis of the clavicle is a rare condition characterized by a defect in the clavicle. Upper limb anomalies have been documented to occur in association with congenital heart malformations. However, there is no documented report of congenital heart malformation associated with congenital pseudoarthrosis of the clavicle.
Methods: We present a 9 year old boy with left clavicular pseudoarthrosis coexisting with tetralogy of Fallot.
Keywords: Congenital Pseudoarthrosis, Clavicle, Holt-Oram syndrome, Tetralogy of Fallot.
Introduction
Congenital pseudoarthrosis of the clavicle is a rare clinical condition characterized by bone defect in the middle of the clavicle. Fitzwilliams first described the condition in 1920; he recognized it as an entity different from obstetric fracture, cranio-cleido dystosis and neurofibromatosis.1 The clavicle develops from two pre-cartilaginous centers as described by Mall (1906), and failure of these nuclei to fuse is believed to result in pseudoarthrosis.2 However, the causes of this failure of fusion is unknown.
Occurrence of congenital pseudoarthrosis of the clavicle in association with congenital cardiac malformation is not documented in the literature. However, several heart-hand syndromes have been identified, with Holt-Oram syndrome being the commonest. These syndromes are believed to be linked by the TBX 5 gene. Holt- Oram syndrome is an autosomal dominant disorder characterize by upper limb abnormalities in association with congenital heart malformation.3 The spectrum of upper limb involvement varies and may involve malformations of the carpal bones, thenar bones, radial bones or shoulder including phocomelia.3 We report a case of congenital pseudoarthrosis of the clavicle in association with Tetralogy of Fallot which has previously not been documented.
Case report
A 9-year-old boy was referred to the Orthopaedic outpatient clinic in our facility on account of left clavicular deformity noticed 13 months prior to presentation. There was no history of trauma to the chest or upper limb. A deformity was noted in the middle third of the left clavicle, it was painless and, more prominent with the arm abducted. There were no obvious skin changes and no functional impairment in the left shoulder. He had been diagnosed to have tetralogy of Fallot with severe right ventricular outflow obstruction at birth. He had a bidirectional Glenn shunt done 2 years prior to presentation and is currently being worked up for definitive heart surgery. There was no family history of congenital anomalies.
A chest radiograph revealed a left clavicular pseudoarthrosis characterized by a defect in the middle of the left clavicle, with a bulbous lateral segment, sclerotic ends with no evidence of callus formation (figure 1). His mother was counselled on the diagnosis and treatment options. She opted for a non-operative treatment modality. He has full range of motion in the shoulder with moderate deformity.
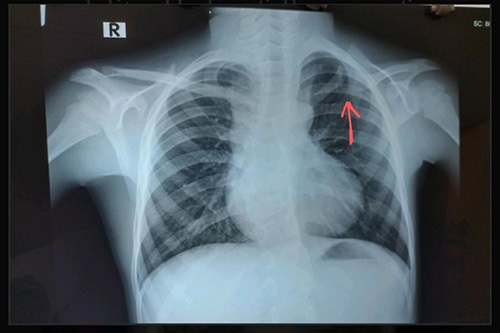
Figure 1
Discussion
About 200 cases of congenital pseudoarthrosis of the clavicle have been reported in the literature.2 Most cases are unilateral and right sided, but in about 10% of cases it occurs on the left in association with other congenital disorders such as dextrocardia.2 The cause of failure of fusion is unknown; however, several hypotheses have been proposed such as excessive pressure exerted by pulsation of the subclavian artery during the process of development of the clavicle and conditions whereby the right subclavian artery lies at a higher level than the left.2 A gene, TBX5 gene is responsible for encoding a transcription factor T-Box 5, which regulates the expression of other genes important in cardiac septation and development of bones in the upper limbs.3 Mutation in this gene can result in upper limb malformations including clavicular pseudoarthrosis and varying degrees of cardiac malformations.
Upper limb anomalies are known to be associated with congenital heart malformations (the Heart–hand syndrome), with Holt-Oram syndrome being the most diagnosed. Holt-Oram syndrome is an autosomal dominant disorder with upper limb abnormalities in association with congenital heart malformation.3 The Holt-Oram syndrome is caused by heterogeneous mutation of TBX5 gene located on the long arm of chromosome 12q24, this gene is responsible for encoding transcriptional factors involved in the development of the heart and upper limbs.3 More than 85% of patients with Holt-Oram syndrome have this mutation, which can be nonsense mutations, deletions, rearrangements, and missense mutations in the TBX5 gene,3,6 while about 40% of cases represent new mutations.4,6,9
In patients with congenital cardiovascular malformation without an identifiable syndrome, about 8.8% have coexisting extra cardiac anomalies involving the musculoskeletal system.5 Cardiac defects are variable and can be as simple as an isolated ostium secundum, atrial septal defects (ASD) or muscular ventricular septal defects (VSD), or multiple and complex malformations.6 Some individuals with familial Holt-Oram syndrome showed only ECG abnormalities such as conduction disorders without structural cardiac anomalies.7 The spectrum of upper limb involvement varies and may involve malformations of the carpal bones, thenar bones, and radial bones up to extreme shortening or absence of the limb.3
Involvement of the shoulders is known to occur with minimal or absent deformity in the hands.8 This feature seems to be specific to Holt-Oram Syndrome and is not seen in cases of isolated radial ray defects. Deformities in the shoulder include a combination of short hypoplastic clavicles, hypoplasia of the head of the humerus, prominence of the lateral third of the clavicle and acromioclavicular joint.7,8 Limb abnormalities characteristically affect the left side more than the right; this is different from other radial ray defects which generally show right sided preponderance.8
Clinically, congenital pseudoarthrosis of the clavicle is identified by a subcutaneous painless swelling around the middle third of the clavicle which becomes prominent when the upper limb is raised and with growth.2 The range of motion of the shoulder is usually normal with no functional impairment.2 Plain radiograph findings include clear separation of the middle third of the clavicle, with the medial segment situated above the lateral segment. The lateral end appears bulbous while the medial end is atrophic, with obliteration and sclerosis of the canal with no feature of callus formation is characteristic.2 These clinical and radiologic findings were consistent with finding in the index case.
Congenital pseudoarthrosis of the clavicle must be differentiated from obstetric fracture, post traumatic non-union, cleido-cranial dystosis and neurofibromatosis. This is usually done from the history and physical examination. Most patients may remain asymptomatic throughout life with no functional impairment and will not opt for any form of treatment.2
Occurrence of musculoskeletal anomalies in patients with congenital heart malformation is not uncommon.4 However, there is no constant association between a specific musculoskeletal anomaly and a particular type of cardiac malformation.4 This creates a large pool of possible combinations that can occur, and hence a high index of suspicion is required to identify this syndrome. Patients with Holt-Oram syndrome may have upper limb deformities with no obvious structural cardiac abnormalities. Clinical recognition of this syndrome will require detailed physical examination and relevant investigations to identify subtle forms of this syndrome. We did not find literature evidence of previous reports of congenital pseudoarthrosis in association with a congenital cardiac anomaly, and we believe that, to the best of our knowledge, this is the first reporting in the literature of this combined anomaly, which we strongly believe is a hitherto unreported variant of the Holt-Oram syndrome.
References
- Fitzwilliams DC. Hereditary cranio-cleido-dysostosis. Lancet 1910; 2:1466-75.
- de Figueiredo, Marina Juliana Pita Sassioto Silveira et al. “CONGENITAL PSEUDARTHROSIS OF THE CLAVICLE.” Revista brasileira de ortopedia vol. 47,1 21-6. 16 Nov. 2015, doi:10.1016/S2255-4971(15)30341-4.
- Krauser AF, Ponnarasu S, Schury MP. Holt Oram Syndrome. 2021 Aug 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. PMID:30020711.
- Ríos-Serna LJ, Díaz-Ordoñez L, Candelo E, Pachajoa H. A novel de novo TBX5 mutation in a patient with Holt-Oram syndrome. Appl Clin Genet. 2018; 11:157-162. Published 2018 Nov 23. doi:10.2147/TACG.S183418
- Holt M, Oram S. Familial Heart disease with skeletal malformations. Br Heart J.1960 Apri;22(2);236-242. doi:10.1136/hrt.22.2.236
- G. Chryssostomidis, M. Kanakis, V. Fotiadou, et al. Diversity of congenital cardiac defects and skeletal deformities associated with the Holt–Oram syndrome Int J Surg Case Rep, 5 (7) (2014), pp. 389-392.
- Newbury-Ecob RA, Leanage R, Raeburn JA, Young ID. Holt-Oram syndrome: a clinical genetic study. J Med Genet. 1996;33(4):300-307. doi:10.1136/jmg.33.4.300.
- Chin J, Pereira S, Camacho A, et al. Holt-Oram syndrome: a case report. Rev Port Cardiol. 2014;33(11): 737.e1–5.
- Huang T. Current advances in Holt-Oram syndrome. Current Opinion in Pediatrics. 2002 Dec;14(6):691-695. DOI: 10.1097/00008480-200212000-00008. PMID: 12436037.
- Abdullah A. Alabdulgader, 2012. Extra Cardiac Anomalies Associated with Congenital Cardiac Malformations in Saudi Arabian Population. Research Journal of Cardiology, 5: 12-19.