Thyroidectomy refusal and long-term anti-thyroid use in toxic multi-nodular goitre
Uwanuruochi K1, Uwanuruochi V2
Abstract
Background: Definitive management for most patients with toxic goitres comprise thyroidectomy or radioiodine ablation.
Method: We report a middle aged woman who refused surgery on personal grounds, and in the absence of radioiodine was managed long-term with oral anti-thyroid.
Results: The clinical outcome was fair.
Conclusion: Our study, the first report of long-term anti-thyroid use from our centre, highlight the peculiarities of management under this scenario.
Keywords: Thyroidectomy refusal, long-term anti-thyroid, toxic multi-nodular goitre.
Introduction
There are reports of varied efficacy for long-term anti-thyroids in treating toxic nodular goitre. Our case report highlights the possibility of good outcome, the problems associated with this treatment regimen, and precautions that should be taken when patients refuse the standard regimen, or they are not affordable.
Case report
OA, a 46 year old female, first attended our facility seven years ago with a four year history of disfigured left finger nail, associated with crumb formation and nail separation and was treated for onychomycosis. She also developed palpitations, with restlessness and poor sleep, headache and neck pain. She was hypertensive for one years and was on treatment with amlodipine. A year later, she had developed diabetes and took metformin and glybenclamide sparingly and two years later, she developed a neck swelling and was diagnosed as a simple goitre (Figure 1).

Figure 1: Multi-nodular goitre
Blood pressure was about 150/90mmHg, with pulse rate of 84/minute. A neck ultrasound revealed a multi-nodular goitre. Both glands were enlarged, the right measuring 52.4mm by 23.2mm by 34.6 mm, giving a volume of 20 ml, the left measured 56.5mm by 27.6mm by 44mm, volume 35.8ml (Figure 2). There were multiple echogenic nodules, the average dimension on the right being 2.14cm by 1.64 cm, and on the left 1.40cm by 1.77cm.
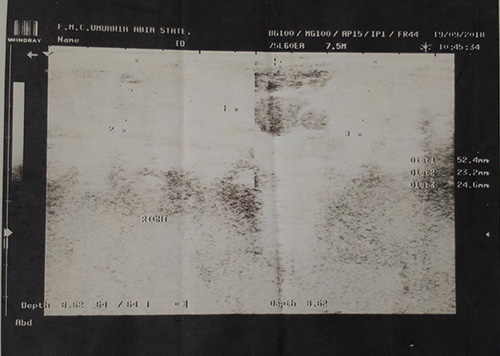
Figure 2 Initial ultrasound scan
Four years later, on repeat ultrasound scan, the largest nodule on the right was 2.32cm by 1.9 cm, that on the left 2.4cm by 1.9 cm (Figure 3). No enlarged cervical lymph nodes were seen.
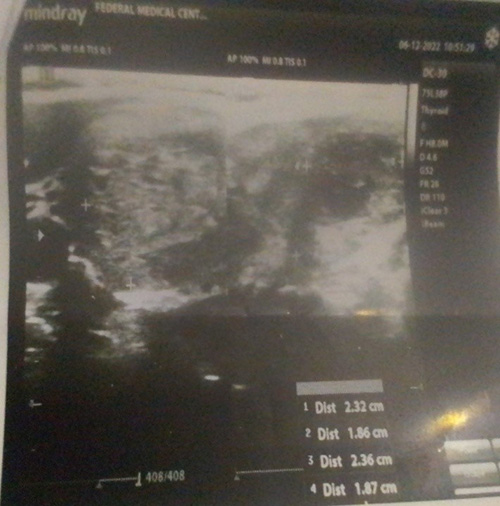
Figure 3 Repeat Ultrasound scan
The baseline ECG was not available but a recent ECG showed a normal sinus rhythm (Figure 4).
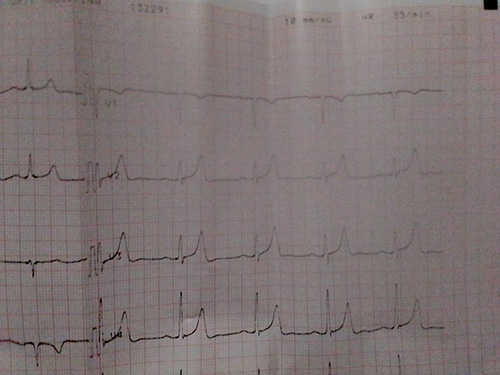
Figure 4 Normal sinus rhythm
Table 1: Serial thyroid function results

Blood sugar tests were normal. Serial thyroid function tests results are shown below (Table 1)
An impression of toxic multi-nodlular goitre was made and she was place on Carbimazole 15mg tds, alongside metoprolol 25mg bd and lisinopril 5mg daily. Normal thyroid hormone levels were achieved four years ago, but the patient rejected thyroidectomy, having lost her mother-in-law post thyroidectomy. Her anti-thyroid medication was reduced to 5mg tds when symptoms abated, but she took it irregularly. Current anti-hypertensives are carvedilol 12.5 mg daily and losartan 100mg daily.
Discussion
This unique case presents a dilemma to the physician. Apart from unwillingness to undergo surgery, there was also poor compliance with treatment. However, the patient experience clinical as well as laboratory remission following long-term though irregular carbimazole use.
Standard current recommendation for toxic multi-nodular goitre comprises surgery, whereas anti-thyroid drugs are used to achieve euthyroidism, followed by near-total thyroidectomy and thyroxine replacement and radioiodine ablation.1 In this case where a patient refuses surgery, and radioiodine ablation was not available, the option left for the physician is long term use of anti-thyroid medication.
Such patients should be well informed about the risk of long term anti-thyroid. However, various studies have given various levels of support for long-term antithyroids.2-5 There are reports of good efficacy and safety, hence its recommendation as an alternative treatment for toxic multi-nodular goitre.
It has been observed that a much smaller percentage of those taking anti-thyroid drugs developed hypothyroidism, compared to patients treated with radio-iodine or surgery.6 However patients should be counselled that antithyroid do not usually produce permanent remission.7 They should also be informed of the potential but serious even though rare side effect of agranulocytosis. Attention has also been drawn that favourable candidates for anti-thyroids are young, have small goitres or goitres which regress during treatment, and have mild hyperthyroidism of short duration.8 All these appeared to have weighed into our patients favour.
Compliance remains a problem which should be addressed to reduce frequency of relapses. Single daily dosing, which has been recommended by Gupta et al9 will help in this regard. Carbimazole has advantage in this over methimazole because of its longer half-life.10
Our case highlights an often ignored indication for long-term anti-thyroid medication, patient unwillingness to undergo surgery, as well as some of the challenges of anti-thyroid drugs. Our index patient improved with suboptimal compliance to anti-thyroid medication. The problems of long-term anti-thyroid administration should be appreciated, and precautionary measures taken.
References
- Porterfield JR Jr, Thompson GB, Farley DR, Grant CS, Richards ML. Evidence-based management of toxic multinodular goiter (Plummer's Disease). World J Surg. 2008 Jul;32(7):1278-84. doi: 10.1007/s00268-008-9566-0. PMID: 18357484.
- Azizi, F., Malboosbaf, R. Safety of long-term antithyroid drug treatment? A systematic review. J Endocrinol Invest 42, 1273–1283 (2019). https://doi.org/10.1007/s40618-019-01054-1
- Malboosbaf R , Azizi F. Long-Term Treatment with Antithyroid Drugs: Efficacy and Safety. Int J Endocrinol Metab.18(Suppl):e101487. doi: 10.5812/ijem.101487.
- Hershman JM, Givens JR, Cassidy CE, Astwood EB. Long-term outcome of hyperthyroidism treated with antithyroid drugs. J Clin Endocrinol Metab. 1966 Aug;26(8):803-7. doi: 10.1210/jcem-26-8-803. PMID: 4162249.
- Azizi F, Takyar M, Madreseh E, Amouzegar A. Treatment of Toxic Multinodular Goiter: Comparison of Radioiodine and Long-Term Methimazole Treatment. Thyroid. 2019 May;29(5):625-630. doi: 10.1089/thy.2018.0397. Epub 2019 Apr 23. Erratum in: Thyroid. 2019 Dec;29(12):1871. PMID: 30803411.
- Bawand R, Borzouei S, Salimbahrami SA, Sheikh V. Comparison of clinical efficacy of antithyroid drugs, radioactive iodine, and thyroidectomy for treatment of patients with graves' disease, toxic thyroid adenoma, and toxic multinodular goiter. Biomed Biotechnol Res J 2022;6:569-75
- van Soestbergen MJ, van der Vijver JC, Graafland AD. Recurrence of hyperthyroidism in multinodular goiter after long-term drug therapy: a comparison with Graves' disease. J Endocrinol Invest. 1992 Dec;15(11):797-800. doi: 10.1007/BF03348807. PMID: 1283983.
- Hamburger, J.I. (1981). Is Long-Term Antithyroid Drug Therapy for Graves’ Disease Cost-Effective?. In: Hamburger, J.I., Miller, J.M. (eds) Controversies in Clinical Thyroidology. Springer, New York, NY. https://doi.org/10.1007/978-1-4612-5916-9_5
- Gupta SK, Mithal A, Godbole MM. Single daily dose of carbimazole in the treatment of hyperthyroidism. Natl Med J India. 1992 Sep-Oct;5(5):214-6. PMID: 1302580.
- Cooper DS. Antithyroid Drugs. N Engl J Med 2005;352:905–17.