Comparative evaluation of predictors of dental caries among adult population in a metropolitan city in North West Nigeria: A case-control study
Sotunde OA1, Iliyasu Z2, Idon PI3, Akinboboye BO4, Ikusika OF1, Makanjuola JO4, Enone LL5, Alalade O1, Igweagu CE1
Abstract
Background: Dental caries as a disease entity has not been eradicated but controlled worldwide. The predictors of dental caries play a significant role in the holistic approach in the management of dental caries. The aim of this study is to evaluate the predictors of dental caries among adult population in North West Nigeria.
Material and Methods: The study populations consist of adults between 20-60 years old, with diagnosis of dental caries (case) and those without dental caries (control), both were confirmed after intraoral examination. A multistage sampling technique was employed to select the study respondents. Mouth mirror and caries explorer (dental probe) were used for intraoral examination to confirm diagnosis of dental caries. An initial calibration of the research assistants was done on intraoral examination by the principal researcher, assessing the same respondents examined by the research assistants. Data was analyzed using SPSS Statistical software version 20.0.
Results: The older age groups were 4% less likely to have caries (p <0.001, AOR= 0.96, 95% CI =0.94-0.98) while participants that took local sweet drinks were 2.8 times more predisposed. Respondents without scaling and polishing were 4.8 times more likely to have caries (p=0.01, AOR= 4.82 95% CI=1.45-16.05) while those who received oral hygiene instructions were 72% less likely to have caries (p<0.001, AOR=0.28 95% CI= 0.11-0.67).
Conclusion: Age, family history, teeth cleaning method, use of fluoride toothpaste and source of oral health maintenance were found to be independent predictors of dental caries.
Introduction
It is estimated that oral diseases affect approximately 3.5 billion people worldwide.1 Despite research and clinical efforts, the prevalence of oral diseases such as dental caries is still rising in many parts of the world. According to World Health Organization (WHO), untreated dental caries in permanent teeth is the most common health condition.2 The goal of WHO on severity of dental caries keep changing based on the need to minimize cases of dental caries recorded in different geopolitical zones globally.3 However, it must be emphasized that dental caries as a disease entity has not been eradicated but only controlled worldwide due to continuous exposure of certain percentage of the population to both clinical and general predictors.3 The clinical identifiable predictors include tooth structure, morphology, malocclusion, fluoride content of the tooth/saliva and salivary rate4 while general predictors of dental caries include age, sex, race, socioeconomic status, culture, lifestyle, genetic factors, maternal health, nutrition and geographical differences.5 The general predictors can be classified as either proximal or distal. The proximal level is related to age, sex, race and modifiable behavior such as oral hygiene practices, dietary habits, life style and the use of oral health services while the distal level is related to socio-economic and environmental factors such as the availability of oral health services.5
The predictors of dental caries play a significant role in the holistic approach in the management of dental caries in order to reduce incidence of dental caries among population. Many a times, the planning of oral health services is often oriented towards clinical services but in developing country not many in the society present for dental check-up nor report at early stage of oral diseases, particularly at the incipient stage of dental caries when the pain is still bearable.
Moreover, it is imperative to explore the role of the aforementioned multifactorial predictors in patient accessibility to dental services. This is a case-control study which explored the effects of general predictors of dental caries among adult population in Kano, a metropolitan city with largest population in Northern part of Nigeria. Most studies on dental caries in Sub-Saharan Africa focus on children while in reality adults are not excluded in the prevalence of dental caries in both developed and developing countries. Furthermore, the few available literatures on adult caries are cohort studies which did not compare the effects of predisposing factors on participants with and without dental caries. The aim of this study is to evaluate the predictors of dental caries among adult population in Kano metropolis, a commercially dynamic population in North West Nigeria.
Methodology
The study was a case-control study which was commenced after the ethical clearance was obtained from the Ministry of Health, Kano State. The study populations consist of adults between 20-60 years old, with diagnosis of dental caries (case) and those without dental caries (control), both were confirmed after intraoral examination. An informed consent was obtained from each participant before commencement of the study. Exclusion criteria for cases and controls include adults that withhold consent to the study, those too sick particularly to participate in the study i.e those that cannot withstand the rigor of thorough intraoral examination due to debilitating/ chronic disaeses or adults with reduced salivary flow rate (dry mouth). The sample size was determined using the case-control formula6 resulting in 175 subjects in each group after making provision for attrition rate and these were recruited for the study. A multistage sampling technique was employed to select the study respondents. Two Local Governments Areas (LGA), Kano Municipal and Tarauni, were selected from the list of 8 LGA in Kano Metropolis. Two political wards were selected from each LGAs. For Kano Municipal LGAs, Zango and Yakasai wards were selected while Unguwa Uku and Gyadi Gyadi Kudu were selected for Tarauni LGAs. Twenty-five percent of the settlements were selected from each sample ward. Sample size allocated to the two selected wards was proportionate to the population size of the settlements. In each of the wards a calculation was done to determine what constitute the 25% of the total settlements and this was rounded up to nearest whole number. Systematic sampling technique was used to select individual respondents in each ward. Enumeration area of the households was used and serial numbers allocated to obtain the sampling frame. To obtain a starting point, simple random sampling (using random number table) was used to select the household corresponding to a number between 1 and the sampling interval. Subsequent households were identified by adding the sampling interval to the preceding household serial number. In the household with more than one eligible respondent one was selected using a simple one time/point ballot. This was continued until the sample size was achieved.
An interviewer administered semi-structured questionnaire was adapted from the study on development of a model to assess community level risk of oral diseases7. Wooden spatula, mouth mirror and caries explorer (dental probe) were used for intraoral examination to confirm diagnosis of dental caries. The data collection required sixteen research assistants to accomplish the work within the stipulated time frame. The research assistants were oral health care workers with minimum qualification of Dental Surgeon Assistant (DSA) certificate. There were four teams, each team is made up of two dental surgeons (male and female) and two DSAs (male and female). This allowed for cultural sensitivity as some men do not allow male to interview their wives. An initial calibration of the research assistants was done on intraoral examination by the principal researcher, assessing the same respondents examined by the research assistants. The DMFT scores after intraoral examination by each examiner was recorded and compared. The inter examiner consistency was determined by calculating the Kappa (k)8 statistics. The Kappa coefficient calculated for this study ranged from 0.93 to 1.00. All research assistants were fluent in Hausa (community language), trained on questionnaire administration and intraoral examination. DMFT Index was used to score dental caries.
Data analysis
Data was analyzed using SPSS Statistical software version 20.0. Socio-demographic variables of respondents were calculated and presented using mean, frequencies and percentages for quantitative variables. Dental caries was the dependent variables while the independent variables include socio-demographic data, oral hygiene practices, dietary habits, socioeconomic factors and utilization of dental services by the respondents. A Chi-square test or the Fisher’s exact test (where appropriate) was used to analyse factors associated with dental caries in the respondents. In all tests of significance, P<0.05 was considered statistically significant. At multivariate level, logistic regression analysis was used to obtain crude and adjusted odds ratio with 95% confidence intervals for predictors of dental caries.
Results
Among adults’ population with dental caries (cases) 171 of the 175 approached consented to participate in the study while among adults’ population without dental caries (control) 174 of the 175 consented to participate in the study. The response rates were 97.7% and 99.4% respectively.
Table 1: Socio-demographic characteristics of respondents
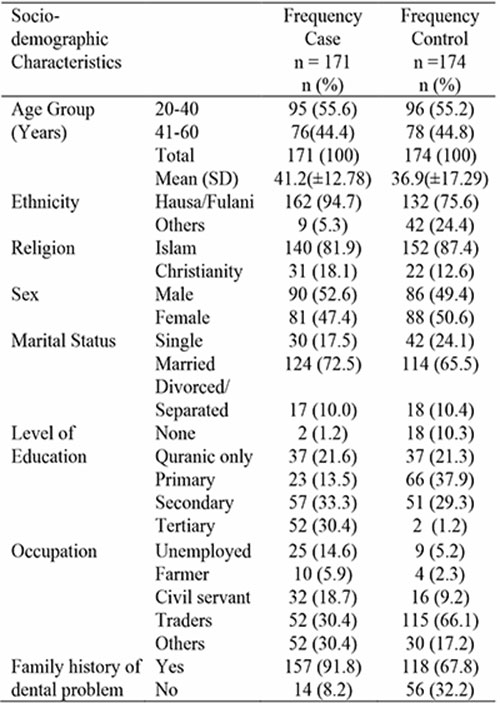
Table 2: Predictors of dental caries (Socio-demographic factors)
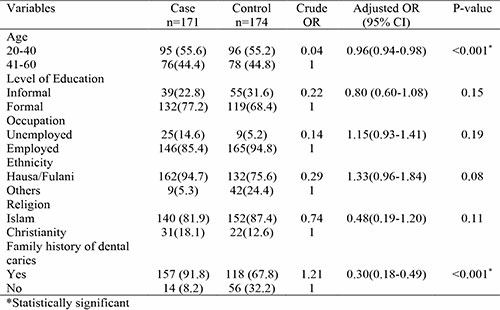
Table 3: Predictors of dental caries (Oral hygiene practices)
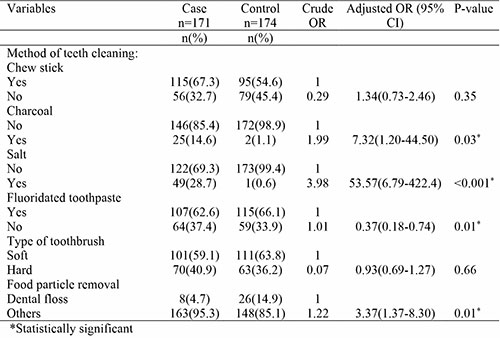
Table 4: Predictors of dental caries (Dietary habits)
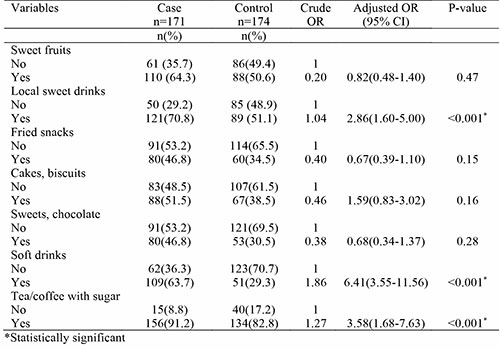
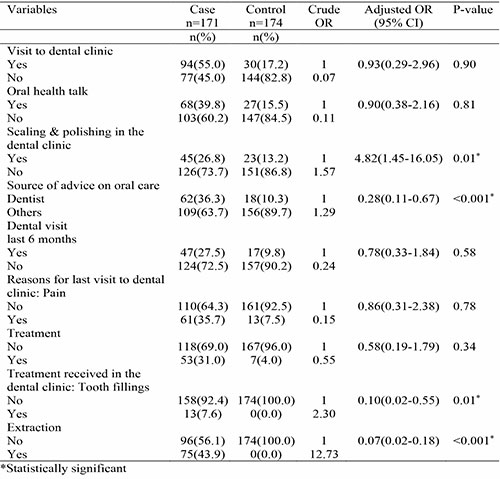
Table 5: Predictors of dental caries (Utilisation of dental services)
Discussion
This study considered predictors of dental caries which include sociodemographic factors, oral hygiene practices, dietary habits and utilization of dental services. In the assessment of socio-demographic factors, age, occupation, level of education and family history of dental caries were found to be significantly associated with dental caries at bivariate level while at multivariate level age and family history of dental caries remain independent predictors of dental caries. The respondents in the 41-60 year age groups were 4% less likely to have caries (p <0.001, AOR= 0.96, 95% CI =0.94-0.98) compared to the younger age groups. This was supported by a study9 conducted by Olabisi et al, which reported the lowest DMFT (caries experience) among age group 55-64 years and highest caries experience among age group 30-34 years. In the United States, Gupta et al10 reported that the odds of untreated caries among adults aged 19 to 45 years were higher than adults aged 45 years and above. This is also similar to a study conducted by Namal et al11 among Turkish adults in which the mean age of the participants was 39.4 years and age range was 18–74 years. According to Namal et al11 the likelihood of developing dental caries decreases with age from 85.0% at age 18–19 years, to 58.2% at 35–44 years and 16.7% at 65–74 years. This is contrary to the study12 carried out in Bulgaria to establish the mean DMFT of adults over the age of 20 years which reported that DMFT index was highest (24.21) among the adults aged 60 years and above, lower (21.22) in the age group of 50–59 year-old, and it was lowest (10.33) in the youngest age group of 20-29 year old. However, the result in this present study could be due to selective patterns of older age group concerning diet, particularly avoiding high sugar content refined food or drinks which are cariogenic. Some older age group avoid these food/drinks to prevent or manage age-related non-communicable diseases such as hypertension, diabetes which indirectly reduce the susceptibility of developing dental caries.
The oral hygiene practices play a major role as risk factors of dental caries. At bivariate level, use of chewing stick, charcoal, salt, fluoridated toothpaste, and method of removing food particles were found to be significantly associated with dental caries while at multivariate level charcoal, salt, fluoridated toothpaste and method of food particle removal remain independent predictors of dental caries. Respondents that use charcoal were 7 times more likely to have dental caries (p=0.03, AOR=7.32. 95% CI=1.20-44.50) while respondents that uses salt were 53 times more vulnerable to have dental caries (p<0.001, AOR=53.57 95% CI=6.79-422.4). Respondents that used wrong methods of food particle removal were 3 times more prone have dental caries (p=0.01, AOR=3.37, 95% CI=1.37-8.30) while respondents that uses fluoridated toothpaste were 63% less likely to have dental caries (p=0.01, AOR=0.37 95% CI=0.18-0.74). This finding is similar to a study carried out by Tafere et al13 in Ethiopia which reported that dental caries was lower among respondents who practiced good oral hygiene measures (AOR = 0.05, 95% CI, 0.02, 0.81). Another study in New York14 indicated that poor oral hygiene and resultant plaque accumulation are associated with increased risk for dental caries in adults. In Norway, Oscarson et al15 reported that the predictors of belonging to ‘caries free’ group, i.e. having zero visual caries signs, increased for individuals who brushed their teeth twice daily, removed food particles with dental floss, drank sugar-containing soft drinks seldom or attended dental services annually. On the type of toothpaste, a study in Belarus16 reported that the prevalence of dental caries among those who use locally made non-fluoridated toothpaste were high (83.1%).
Furthermore, dietary habits as a major primary causative factor in pathogenesis of dental caries showed that intake of sweet fruits, local sweet drinks, fried snacks, cakes/biscuits, soft drinks and tea/coffee with sugar were significantly associated with dental caries at bivariate level while at multivariate level local sweet drinks, soft drinks and tea/coffee with sugar were found to remain independent predictors of dental caries. Respondents that took local sweet drinks were 2.8 times more likely to have dental caries (p<0.001, AOR=2.86, 95% CI=1.60-5.00). Respondents that took soft drinks were 6 times more likely to have dental caries (p<0.001, AOR=6.41 95%CI=3.55-11.56) while respondents that took tea/coffee with sugar were 3.5 times more likely to have dental caries (p<0.001, AOR=3.58, 95% CI=1.68-7.63). This finding was corroborated by a study17 conducted in Enugu, Southeast Nigeria, which reported that dental caries was associated with higher consumption of sugary snacks among respondents. A cross-sectional study18 was carried out in Dawan Valley, a district of the Hadhramaut Province, Yemen. The study included 346 adults aged 18 years old to 68 years old. It reported that factors associated with dental caries include eating habits i.e frequent taking of snacks between meals (AOR=4.59). Studies in United States indicate that frequent snacking, intake of sugary foods, beverages and poor access to preventive dental care services were associated with increased risk for dental caries in adults.14,19
In the subjects’ utilization of dental services, dental caries was found to be significantly associated with visit to dental clinic, oral health talk, scaling and polishing in the clinic, source of advice on oral health (parents, dentist and friends), visit to dental clinic in the last 6months, reasons for visit (pain and treatment) and treatment received in the clinic (fillings, extraction and other treatment). At multivariate level, scaling and polishing in the dental clinic, source of advice on oral care and treatment received in the clinic remain independent predictors of dental caries. Respondents that had no scaling and polishing in the clinic were 4.8 times more likely to have dental caries (p=0.01, AOR= 4.82 95% CI=1.45-16.05) while those who received advice from dentists are 72% less likely to have dental caries (p<0.001, AOR=0.28 95% CI= 0.11-0.67). Respondents who attended dental clinic for other treatment apart from extraction were 93% less likely to have dental caries (p<0.001, AOR= 0.07 95% CI=0.02-0.18). A study20 conducted in Nice, France also highlighted protective factors such as preventive visit to the dentist (OR: 0.63, 95% CI: 0.41–0.99) as predictor of dental caries. Another study16 showed that the prevalence of root caries was 57.7% among adults who visited dental clinics less than once a year while it was 12.7% among those who visited dental clinics more than once a year.
Conclusion
Following evaluation of the predictors of dental caries among adult population in Kano metropolis, age, family history of dental caries, teeth cleaning mode, use of fluoride toothpaste, method of eliminating food interdentally, oral prophylaxis, source of oral health maintenance and treatment received in the dental clinics were found to be independent predictors.
Recommendations: We recommend more awareness to be created on the availability and use of dental floss as the best method of eliminating food particles interdentally.
References
- Global, regional and national incidence, prevalence and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990 – 2017: a systematic analysis for the Global Burden of Disease study 2017. Lancet 2018; 392: 1789 – 8583.
- WHO oral health country/area profile. Geneva: World Health Organisation.2018
- Listl S, Galloway J, Mossey P A, Maecenes W. Global economic impact of Dental Diseases. J Dent Res. 2015; 94(10):1355-61.
- Fejerskov O, Kidd E. Dental caries: the disease and its clinical management. Oxford: Blackwell Mun¬sksgaard; 2008.
- Costal SM, Vasconcelos M, Abreu MHNG. High Dental Caries Among Adults Aged 35-44years: Case-Control Studies of Distal and Proximal Factors. Int J Environ Res Public Health. 2013;10: 2401-11.
- Hajian-Tilaki K. Sample size estimation in epidemiologic studies. Caspian J Intern Med. 2011;2(4):289-98.
- Silva AM, Gkolia P, Carpenter L, Cole D. Developing a model to assess community level risk of oral diseases for planning public dental services in Australia. BMC Oral Health. 2016;16:45.
- McHugh ML. Interrater reliability: The Kappa statistics. Biochemia Medica 2012;22(3):276-82
- Olabisi AA, Udo UA, Bashiru BO. Gbenga OO, Adeniyi AO. Prevalence of dental caries and oral hygiene status of a screened population in Port Harcourt, Rivers State, Nigeria. J Int Soc Prevent Communit Dent 2015;5:59-63.
- Gupta N, Vujicic M, Yarbrough C, Harrison B. Disparities in untreated caries among adults in the US, 2011-2014. BMC. 2018;18:30
- Namal N, Can G, Vehid S, Koksal S, Kaypmaz A. Dental health status and risk factors for dental caries in adults in Istanbul, Turkey. Eastern Mediter Health Journal. 2008;14 (1) :110-18
- Bonev B, Avramova N, Yaneva K, Filchev D. Dental Caries and Associated Socio Demographic Factors in Adult People in Bulgarija Balk. J Dent Med. 2015; 19:33-7
- Tafere Y, Chanie S, Dessie T, Gedamu H. Assessment of prevalence of dental caries and the associated factors among patients attending dental clinic in Debre Tabor general hospital: a hospital-based cross-sectional study. BMC Oral Health. 2018;18:119
- Ahluwalia KP, Cheng B, Josephs PK, Lalla E, Lamster IB. Oral disease experience of older adults seeking oral health services. Gerodontology. 2010;27:96–103.
- Oscarson N, Espelid I, Jonsson B. Is caries equally distributed in adults? A population based cross-sectional study in Norway-the TOHNN-study. Acta Odontol Scand. 2017;75(8):557-63
- Barysenka L. Study of the correlation between risk factors and prevalence of root caries OHDMBSC. 2004;3(4):6-10
- Okoye LO, Ekwueme OC. Prevalence of Dental Caries in a Nigerian Rural Community: A Preliminary Local Survey. Ann Med Health Sci Res 2011;1(2): 187-96.
- Al-Tayar B A, Tin-oo M M. Toombak and other risk factors associated with dental caries among adult males in Dawan Valley, Yemen. J Dent Sci. 2016
- Kim JK, Baker LA, Seirawan H, Crimmins EM. Prevalence of oral health problems in U.S. adults, NHANES 1999-2004: exploring differences by age, education, and race/ethnicity. Spec Care Dentist. 2012;32:234–41
- Ceinos R, Bertrand M F, Cucchi C, Lupi L. Hierarching caries risk factors among first-year university students in Nice (France): a cross-sectional study. BMC. 2017;17:159.