Evaluation of Impacted Canines Utilizing Three Radiographic Methods in Orthodontic Patients in Benin City, Nigeria
Ize-Iyamu IN1,2, Otaren Jn2
Abstract
Background: Impacted canines are one of the most commonly missing teeth in the oral cavity and traditionally, two dimensional (2-D) radiographic views have been utilized in localizing such teeth. The introduction of the 3-D Cone Beam Computed Tomography was to enable localization in three dimensions. A reliable and concise radiographic technique will enable proper diagnosis of the type and extent of impaction and aid in choosing the proper treatment and also monitor treatment progression.
Aim: The aim of this study was to evaluate impacted canines in orthodontic patients utilizing three radiographic methods in Benin City, Nigeria.
Methods: In this prospective study, 34 pre-orthodontic patients (30 with unilateral and 4 with bilateral impactions) and a total number of 38 impacted canines were selected. The Lateral Cephalometric radiograph was used to determine the patients’ orthodontic problem. Three groups of participants were selected and identified based on the radiographic method utilized; with group 1, the periapical / Occlusal group (POCC, n=13); group 2, the Orthopantomogram group (OPG, n=13). The third group was the Cone Beam Computed Tomography group (CBCT, n=12). Impacted canines were detected and the position assessed and classified utilizing three radiographic methods into classes I to VI. The differences between groups and correlations between variables were determined with the student’s t-test and the Spearman correlation coefficient respectively. Significant values of P<0.05 were applied.
Results: The mean age of participants was 18.29±6.15 years. A total number of 30(78.9%) impactions were seen in the upper jaw and 8(21.1%) in the lower jaw. Bilateral impactions were seen in the upper jaw of 3(7.9%) patients and 1(2.6%) in the lower jaw respectively. The position of the canines could only be identified clearly in classes I and II from group 1. Group 2 (OPG) was the least definite in identifying accurately the position of the canines. The CBCT (Group 3) did not record any impaction in the lower jaw. Consecutive paraxial cuts at 1.5mm interval on the CBCT showed the position of the canines to be in Class I in 6(50%), class II in 3(25%) and classes III in 2(16.7%) and VI in 1(8.3%) respectively in the upper jaw.
Conclusion: The CBCT appears to be the most reliable method of identifying the position and depth of impacted canines.
Key words: Impacted canines, periapical x-ray, Occlusal, Orthopantomogram, CBCT
Introduction
Radiographic techniques used in the localization of impacted teeth is an important diagnostic tool which aids in the prognosis and management.1 Numerous techniques have been described and include standard radiographic methods like the periapical, occlusal, Orthopantomogram (OPG), lateral cephalograms and rarely, the CBCT (Cone Beam Computed Tomography) scans. A combination of the first three radiographs gives a 2-D (2 Dimensional) view while the CBCT gives a 3-D (3 Dimensional view).2-5 Although various radiographic exposures including occlusal films, panoramic views, and lateral cephalograms can help in evaluating the position of the canines, in most cases, the periapical and Occlusal films are utilized in our environment.
Periapical radiographs cover a small area and when compared with the occlusal and OPG views which cover a much wider area, is a major disadvantage. Localization of impacted canines can be determined utilizing two Periapical radiographs angulated vertically in different positions; two occlusal radiographs in different horizontal angulations and one OPG combined with a periapical radiograph with the vertical angulation changed. In all these angulations, the x-ray tube is moved either vertically or horizontally.1-5
These methods of combining radiographs1,5 was able to predict the bucco-palatal position of impacted canines with palatally displaced crowns determined in 80%. Other studies have shown that the use of the combined OPG method was however unreliable in the localization of impacted canines.6,7 Studies have shown that frontal and lateral cephalograms may sometimes aid in the localization of impacted canines especially its relationship with other facial structures like the maxillary sinus, infra orbital rim and the floor of the nose.6,8 These views are not usually indicated for routine evaluation of impacted canines but are taken to determine the orthodontic problem which in some cases may show the impacted canines.
The CBCT was also found to be more accurate and reliable in localizing impacted canines than the conventional views, but studies recommended that they should only be used when conventional radiographs cannot provide adequate information.9-11 The CBCT imaging technique utilized in diagnosing impacted canines found an accuracy for localization of these teeth with a range of between 50-90%, while the accuracy from conventional views ranged between 39-85%.9
The most frequently impacted anterior teeth are the maxillary canines with prevalence rates ranging from 0.92%5, 1-2%6,7, 1.5%8 and 2.56%9 for different populations examined. Absence of these teeth which fall within the smile line play a major role in smile aesthetics.4,6 Patients seek orthodontic care to improve their smile and localizing, diagnosing and managing such cases require accurate radiographic images.2-7
There appear to be no studies comparing the reliability of these radiographic methods in localizing the position of impacted canines in our environment. The aim of this study therefore, was to evaluate impacted canines in orthodontic patients utilizing three radiographic methods in Benin City, Nigeria and suggest a suitable method for use in our environment.
Materials and Methods
This cross sectional analytical prospective study was carried out on pre-treatment radiographs of consecutive first time orthodontic patients of the University of Benin Teaching Hospital after obtaining clearance from the ethical committee of the hospital. The inclusion criteria included only those with impacted canines and the clearest resolution and detail on radiographs were analyzed leaving a total sample size of 34. Patients with bilaterally impacted canines were included in the study and the impactions counted as two and recorded as such. This resulted in a total number of 38 impacted canines for the sample size of 34 in this study
Patients with congenital anomalies, medical conditions and a previous history of orthodontic treatment or illnesses were excluded from the study. Children below the age of 14 years were also excluded from the study as the upper canine erupts between the ages of 11-13. The periapical and upper Occlusal radiographs were taken with the same x-ray machine (Belmont DX 073, 2007 model, Japan) while the OPG and lateral cephalometric radiographs were taken by the same radiographic technician and machine in a standardized manner using a digital cephalometric machine (PaX-i-2D imaging system Vatech 2017 PCH-2500 version 2.5.0.) set at x1.25 magnification as recommended by the manufacturer. The images generated were stored directly in the computer data base created using the manufacturer’s software (Dimaxis Pro version 4.1.4; Planmeca, Helsinki, Finland). Conventional measurements were taken using hard-copy printouts of the digital images. The CBCT was taken with the same machine (Carestream CS9300 Select 3-D, 2018 model) by the same radiographic technician, and the impacted canines located using the CS imaging patient browser 7.0.23, Carestream Dental LLC, France. Although previous studies found that slight enlargement may occur when printing hard copies of digital cephalograms, the size difference is minimal and regarded as clinically acceptable.12-14
Method errors of the various cephalometric variables were 1.2° for angular measurements. The systemic error of the two measurements was assessed with the Student’s t test with no significance between measurements. To assess inter and intra-examiner agreement between the position of the impacted canines, a main observer and a second independent observer evaluated all the radiographs at the same time independently and after a 2 week interval. The value of kappa and the strength of agreement was 0.80 and 0.62 respectively for inter-and Intra-examiner agreement indicating a strong agreement.
The study group was divided into three based on the radiographic method utilized:
Group 1: The periapical/Occlusal group (POCC, n=13)
Group 2: The periapical / Orthopantomogram group (OPG, n=13).
Group 3: The Cone Beam Computed Tomography group (CBCT, n=12).
The Lateral cephalometric radiograph was used to determine the skeletal pattern using cephalometric analysis and the measurement of the ANB angle (Point A to nasion to point B) which represents the antero-posterior jaw relationship or the skeletal pattern:
Class I = 2-40
Class II = >50
Class III = <10
Measurement of skeletal and dental problems
SNA, SNB and interincisal angle were assessed using the Steiner analysis15.
SNA- Sella –Nasion- A point (the innermost and concave part of the bony maxilla) to determine maxillary prognathism or retrognathism:
Nigerian values16 of 82-890 were regarded as a normal maxilla
Values of < 810 were regarded as a retrusive maxilla and >900 as maxillary Prognathism16
SNB- Sella –Nasion- B point (the innermost and concave part of the bony mandible) to determine mandibular prognathism or retrognathism:
Nigerian values16 of 79.5-85.90 were regarded as a normal mandible
Values of < 79.40 were regarded as a retrusive mandible and >860 as mandibular prognathism16
Interincisal angle- being the angle formed between the upper and lower incisors:
Nigerian values of 108-1160 were regarded as normal
Values of < 1070 were regarded as bimaxillary protrusion and >1170 as bimaxillary retrusion16
Methods of analyzing the impacted canines
Chaushu’s method17 was used for the periapical, Occlusal and OPG
CBCT: Consecutive single and double parallel paraxial cuts to show the vertical and bucco-lingual relationships were done at an interval of 1.5mm
The impacted canines were then evaluated and classified using the method described by Archer
Classification of impacted canines according to their position and axial inclination
Class I: Maxillary canine in palatal position. This can be horizontal, vertical or angulated.
Class II: Buccally or Labially impacted canine which may be horizontal, vertical or angulated.
Class III: Impacted canine with crown on the palatal side and root on the buccal side or vice versa.
Class IV: Vertically impacted canine between the lateral incisor and first premolar.
Class V: Impacted Canine in the edentulous maxilla.
Class VI: Maxillary canines in unusual or aberrant positions. An example: in the naso-antral wall or infra-orbital margin.
Statistical Analysis
The differences between groups and correlations between variables were determined with the student’s t-test and the Spearman correlation coefficient respectively. P values of <0.05 were accepted as significant.
Results
Table 1: Age distribution of impacted canines according to axial inclination
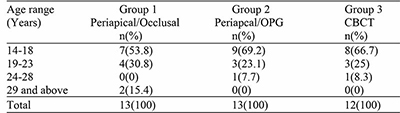
Table 2: Mean distribution of patient’s cephalometric values
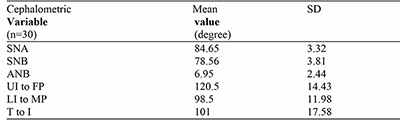
Table 2 indicates the mean cephalometric values of the participants with an increased mean ANB (representing the skeletal pattern) of 6.95±2.440 and a reduced interincisal angle of 1010.
Table 3: Evaluation of the position of impacted canines with 3 radiographic methods
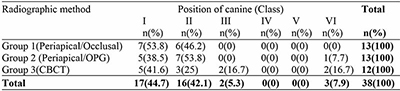
Fig 1: Type of impaction in upper or lower jaw
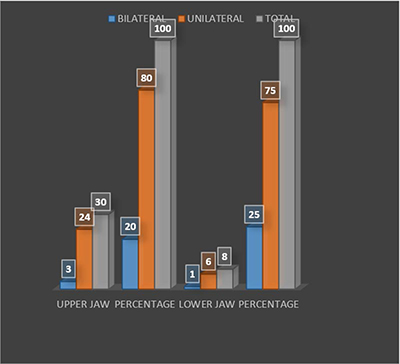
Figure 1 demonstrates the type of impaction in the upper and lower jaws with the unilateral variant being more prevalent in the upper jaws in 24(70.6%), while the bilateral being more prevalent in the upper jaws in 3(8.8%).
Figure 2: Position of impacted canine in jaws
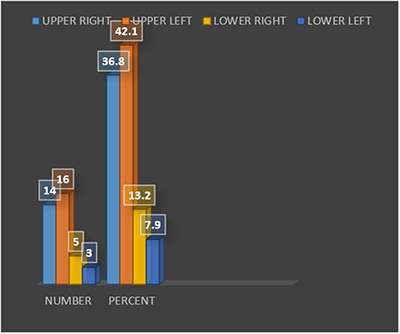
Figure 2 shows the frequency and position of the impacted canines within the jaws. In the upper jaw, a total number of 30 impacted canines were seen with the impacted canine more prevalent on the left in 6 (20%), while in the lower jaw a total number of 8 impacted canines was seen more on the right side in 5(62.5%).
Figure 3: Periapical radiograph showing impacted canine
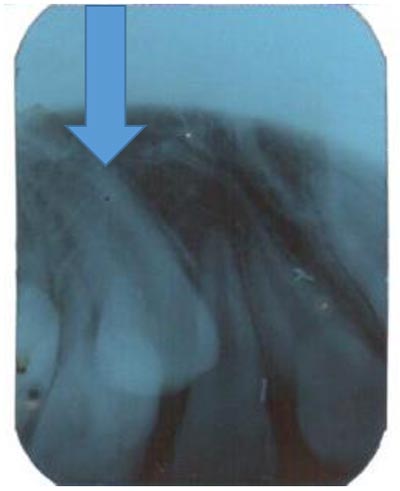
Figure 4: Upper Occlusal radiograph showing bilaterally impacted canines

Figure 5: OPG showing bilaterally impacted canines
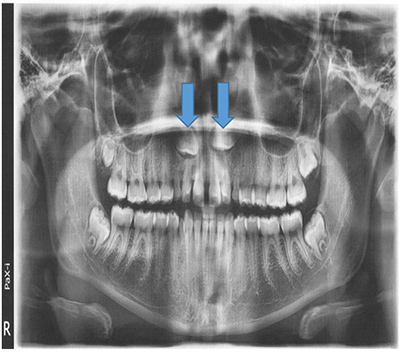
Figure 6: Lateral Cephalogram with tracing for analysis of malocclusion and also showing an impacted canine (arrowed)
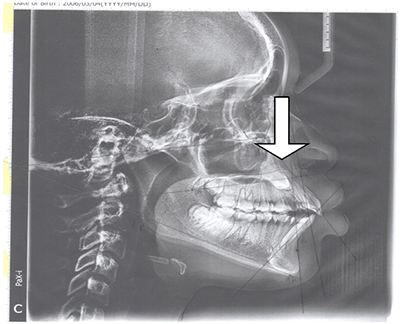
Figure 7: OPG showing impacted canine in class II position, close to floor of maxillary antrum
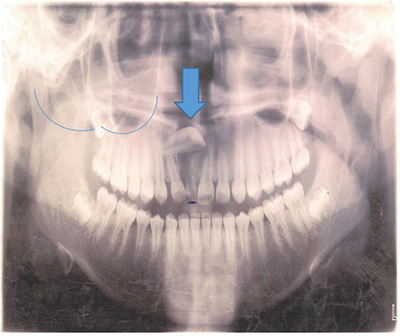
Figure 8: CBCT image showing impacted bilateral canine in a class II position
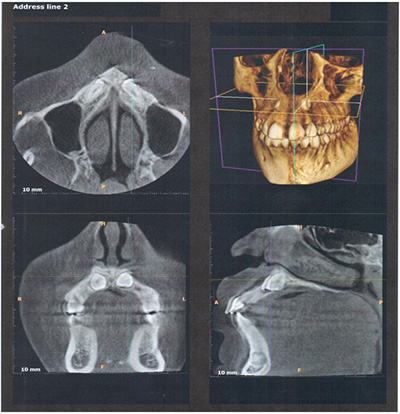
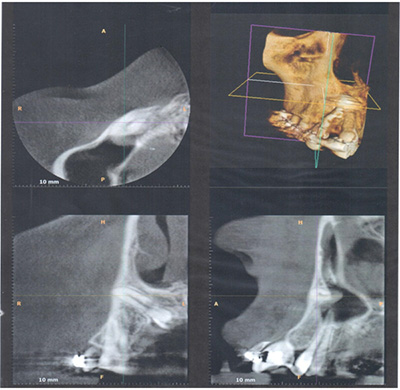
Figure 9: CBCT image showing unilateral impacted left canine in a class III position
Out of the 120 questionnaires given out only 118 was completely filled and analyzed.
There was a total number of 34 patients with 22(64.7%) female and 12(35.3%) male. A total number of 38 impactions were seen. Bilateral impaction was seen in 4 patients (11.8%), with all in females. The mean age of the participants was 18.29±6.15.
Table 1 shows the age distribution of participants with the three different radiographic methods. All three methods had the 14-18-year-olds as the highest number requiring radiographs. The older age group of 24-28years old and above had the lowest number of radiographs taken.
Discussion
The position of impacted canines can be evaluated radiographically utilizing either 2-D or 3-D, single or combined radiographs.1,2,8,9 While a combination of radiographs such as the periapical and occlusal (Group 1) or the periapical and the Orthopantomogram (Group 2) radiographs are common and beneficial in determining the position of impacted canines1,5 This study found out that the position of the canines utilizing the combinations above was useful in classes I (palatally placed) and II (buccally placed) and could also determine the axial inclination as either vertical, horizontal or angulated. This study also showed that a higher number of impacted canines are located either in class I (palatally) or class II (buccally). This is in agreement with other studies2,3,7,8 where the palatally or bucally placed canines were the easiest to locate using either 2-D or 3-D radiographs.
This study did not reveal any impacted canine in class III for groups 1 and 2. However the CBCT (group 3) was reliable in determining the actual position of impacted canines in class III (Impacted canine with the crown on the palatal side and root on the buccal side or vice versa). CBCT studies1,7-12,14 have shown that impacted canines in difficult positions are better and more accurately located with 3-D imaging. Studies by Kumar et al7 demonstrated that conventional 2-D radiographs superimpose structures making it difficult to distinguish fine details and hence reduction in the clarity of the impacted canines. Other studies8-14 showed that 3-D views reveal the exact position of both the crown and root apex and also the orientation, proximity to adjacent teeth and other anatomic structures and the presence of any associated pathologies.10
None of the three radiographic groups evaluated the vertically impacted canines located between the lateral incisor and first premolar (class IV). This could be due to the fact that this position of impaction is uncommon.1,10 Impacted canines in the edentulous maxilla, class V was not seen while utilizing the 3 radiographic methods. This is because all subjects recruited for this study were dentate patients undergoing orthodontic treatment. Studies have shown that orthodontic treatment for impacted canines require radiographs which are useful in establishing the position of these anterior teeth and also in determining management within the bone to a functional state within the oral cavity.4,6,9,18
The maxillary canine located in an unusual or aberrant positions like the naso antral wall or infra-orbital margin (class VI) was seen utilizing the combination of the periapical/OPG (group 2) and the CBCT. The Cone Beam Computed Tomography (CBCT) from the results of this study was able to demonstrate the position of impacted canines in more detail for this group. Superior diagnostic imaging has been identified with the CBCT with the ability to view the images transversely, antero-posteriorly and sagittally.10-14 Studies18,19 demonstrated the advantages of paraxial cuts for better ease of clarity and utilized intervals of 1.5mm to determine fine details of impacted teeth.
The results from this study showed a relatively young age group of 18.29±6.15-years. This is attributable to the fact that aesthetics has become a major reason for seeking orthodontic care especially in the anterior region of the mouth.20 Older patients who have lived with a condition for a longer period appear to be more accepting of the malocclusion than the younger age groups.21
Impacted canines may be unilateral or bilateral and while the group 1 and 2 radiographic groups from this study identified the presence of these teeth, it was almost impossible to determine the position either as buccal or palatal or even the inclination. The group 3 (CBCT) was able to locate the axial inclination, root position and any aberration from this study thus giving superior diagnostic clarity.
The results from this study demonstrated that the upper left quadrant had a higher number of impacted canines when compared with other quadrants.
The mean cephalometric values from the participants with impacted canines in this study showed normal SNA, SNB, upper incisor to Frankfort plane and a normal lower incisor to mandibular plane angle. However, the ANB which represents the skeletal pattern was increased and the interincisal angle which represents the relationship between the upper and lower incisors was reduced with a value of 1010 (degree of bimaxillary proclination). Numerous studies have demonstrated a high prevalence of bimaxillary proclination among Nigerians16,22-24 seeking orthodontic care. Studies have shown that orthodontic problems are also associated with varying cephalometric findings as each patient presents with a problem list unique to them.20
Conclusion
- The periapical/occlusal radiographic combination (Group 1) and the periapical/OPG (Group 2) could determine the position (palatally and buccally placed).and axial inclination (horizontal, vertical or angulated) in classes I and II
- The CBCT (Group 3) was reliable in identifying canines in class III (impacted canines with the crown on the palatal side and root on the buccal side or vice versa)
- Class VI (maxillary canines in unusual or aberrant positions like the naso-antral wall or infra-orbital margin) was identified in groups 1 and 3 but was clearer in detail and accuracy in group 3 (CBCT).
References
- Surej Kumar LK, Nikhil MK, Adersh GA, Mathew T. Techniques for localization of impacted maxillary canine’s radiographs: A new classification system based on the principles of localization. Int J Clin Diag Res 2018;6 (1):1-11.
- Fox N, Fletcher G, Horner K. Localizing maxillary canies using dental panoramic tomography. Br Dent J 1995;179: 416-420.
- Neshlihan ES, Gizem K, Derya Y, Mine C. The reliability of panoramic radiographs in evaluation of location for impacted maxillary canine teeth: comparison of prediction methods. JCDR 2019;13 (7):18-24.
- Grybiene V, Juozenaite D, Kubiliute K. Diagnostic methods and treatment strategies of impacted maxillary canines: A literature review. Somatologija Baltic Dent Maxillofac J 2019; 21 (1):3-12.
- An S, Wang J, Li J, Cheng Q, Jiang CM, Wang YT et al. Comparison of methods for localization of impacted maxillary canines by panoramic radiographs. Dent maxillofac Radiol 2013; 42: 20130129.
- Manne R, Gandikota CS, Juvvadi SR, Rama HR, Anche S. Impacted canines: Etiology, diagnosis and orthodontic management. J Pharm Bioallied Sci 2012; 4 (Suppl 2):S234-S238.
- Kumar S, Mehrotra P, Bhagchandani J, Singh A, Garg A, Kumar S et al. Localization of impacted canines. J Clin Diagn Res 2015; 9 (1):11-14.
- Al-Omar AF, El Dakrory UA. Cone beam computed tomography for evaluation of impacted supernumerary teeth. Oral Health Care 2017; 2(4):1-2.
- Al Qerban A, Jacobs R, Van Keirsbilck P, Aly M, Swinnen S, Fieuws S et al. The effect of using CBCT in the diagnosis of canine impaction and its impact on the orthodontic treatment outcome. J Orthod Sci 2014; 3 (2): 34–40.
- El-Khateeb SM, Arnout EA, Hifnawy T. Radiographic assessment of impacted teeth and associated pathosis prevalence; Pattern of occurrence at different ages in Saudi male in Western Saudi Arabia. Saudi Med J 2015; 36 (8): 973–979.
- Agrawal JM, Agrawal MS, Nanjannawar LG, Parushetti AD. CBCT in orthodontics: the wave of future. J Contemp Dent Pract 2013;4 (1):153-157.
- Polat-Ozsoy O, Gokcelik A, Memikoglu UT. Differences in cephalometric measurements: a comparison of digital versus hand-tracing methods Eur J Orthod 2009; (31): 254–259.
- Enshan ER, Hamid B, Abramovitch K, Kim J. Cone–beam computed tomography vs conventional radiography in visualization of maxillary impacted canine localization. A systematic review of comparative studies. Am J Orthod Dentofac Orthop 2017;151 (2) :248-258.
- Adams GL, Gansky SA, Miller JA, Harrell WE, Hatcher DC. Comparison between traditional 2-dimensional cephalometry and a 3-dimensional approach on human dry skulls. Am J Orthod Dentofac Orthop 2004;126 (4): 377-409.
- Steiner CC. The use of cephalometrics as an aid to planning and assessing orthodontic treatment. Am J Orthod 1960; 46: 721–735.
- Isiekwe M. A cephalometric study of incisor angulations in an Nigerian population. Br J Orthod 1989;163 (3):177-181.
- Chaushu S, Chaushu G, Becker A. Reliability of a method for the localization of displaced maxillary canines using a single panoramic radiograph. Clin Orthod Res 1999;2:194.
- Becker A .Orthodontic treatment of impacted teeth. (3rd ed) Wiley-Blackwell Publishing Co, 2012 Pp, 11-28.
- Scarf WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am 2008:52 (4):707-730.
- Ajayi EO, Ize-Iyamu IN. Malocclusion and occlusal traits amongst orthodontic patients seen at the University of Benin teaching Hospital. Nig Dent J 2010;18 (1):12-16.
- Kang J, kang K. Effect of malocclusion or orthodontic treatment on oral health related quality of life in adults. Korean J Orthod 2014;44 (6):304-311.
- Ifesanya U. An Update on Cephalometrics among Nigerians: Ascertaining Prevalent Jaw Patterns. J Med Med Res 2014; 4(16): 3092-3100.
- Isiekwe M. A cephalometric study of incisor angulations in an Nigerian population. Br J Orthod 1989;163 (3):177-181.
- Ize-Iyamu IN. Comparing sella turcica shapes and dimensions in skeletal classes I, II and III Bimaxillary protrusion patients in a Nigerian population. Ibom Med J 2018; 11 (2) 53-59.