COVID-19 Vaccination: Infectivity and Symptomaticity of SARS- COV-2 among residents in Bonny Island, Rivers State, Nigeria
Ogbondah BO, Owhonda G, Luke A, Jaja ID, Green P, Pius OM
Abstract
Background: In December 2019, the severe acute respiratory syndrome Coronavirus 2 (SARS-COV-2) popularly called COVID-19 emerged. The disease is associated with asymptomatic, mild to severe respiratory symptoms. Use of Vaccine is essential in its control and in Bonny Island, the AstraZeneca chAdOx 1 novel Coronavirus 2019 vaccine was used. Study objective is to determine the effectiveness of this vaccine in preventing infection and symptoms associated with the virus on residents of Bonny Island.
Method: Study is a facility based cross-sectional study, conducted between May and October 2021, at General Hospital Bonny, a COVID 19 testing and vaccination center. Study population were respondents who had previously been vaccinated for Covid-19 that visited the facility for COVID-19 PCR test. All eligible respondents were enlisted into the study until the sample size of 623 was achieved. Interviewer administered questionnaire was used to collect information on socio-demographics and medical history including vaccination status. Multivariate regression analysis using SPSS version 21.0 was used to analyze data with statistical significance set at 0.05. Ethical clearance and permission for the study were granted by appropriate authority while informed consent was extracted from respondents.
Result: There was statistically significant association between COVID-19 vaccination and negative COVID-19 PCR test result (OR 5.98), married couple and age (0-20 and 21-30 years the most and least compliant respectively). There was no significant relationship between symptoms associated with COVID-19 infection and vaccination status.
Conclusion: COVID-19 vaccination uptake protects against COVID 19 infection but does not have any significant effect on symptoms associated with the infection. Married couple and respondents aged 0-20 years were more compliant to vaccine uptake.
Keywords: COVID-19, vaccination, symptoms.
Introduction
The Covid-19 pandemic which resulted from a viral pneumonia of unknown etiology emanated from the city of Wuhan Eastern China in December 2019.1 It resulted in worldwide disruption of business, tourism, health and educational activities.2 The novel Coronavirus disease 2019 (Covid-19) was caused by severe acute respiratory syndrome coronavirus-2 (SARS – COV-2).3 The virus predominantly affects the lungs and transmitted via respiratory droplets of an infected person when they cough or sneeze.4 The clinical presentation of the disease includes fever, cough, shortness of breath, loss of smell and taste sensation. Others include pneumonia, multiple organ failure and death.5 The severe/critical form of the disease which can lead to death occurs in 19.1% of infected person while the mild form which can also present with no symptoms occurs in 80.9% of affected person.6 Treatment for this disease have not been well established and documented, therefore prevention remains the main strategy to contain the pandemic. In Nigeria, the Federal Government together with various States initiated several mechanisms and also activated the National Emergency Operation Center (EOC) which was responsible for the National Public Health response to Covid-19 outbreak in Nigeria. Several preventive mechanisms were recommended by health authorities, however the most viable was the use of vaccine. Health authorities consider vaccination as the most viable methods to contain the pandemic. Covid-19 vaccine have been amazing, achieving impressive outcomes, resulting in attainment of herd immunity.7 However, several encumbrances associated with the vaccine has resulted in poor vaccine acceptance and uptake. widespread misinformation about the vaccine has resulted in vaccine resistance leading to massive dissemination of the infection.8 Study found that 11% of participants view vaccine as more dangerous than the disease they intend to prevent.9 Systemic reviews involving seven million individuals, reveals wanning immunity against SARS-COV-2 infection from high 83% at one month to 22% at five months post vaccination.10 Also temporal wanning of vaccine effectiveness against SARS-COV-2 infection raises concern that initially effective vaccination strategies will not significantly mitigate the individual and population level Covid-19 infective in the long term.10 In addition, confirmed emergence of new variants of the virus threatens to overturn the significant successes achieved in halting the spread of the disease.11 Furthermore, on record, based on epidemiological update by World Health Organization (WHO), as at December 2021, five SARS-COV-2 variants of concern (VOC) and eight variants of interest (VOI) Have been established.12 Due to genetic capability of these variants that enhances their ability to cause severe disease, immune escape, transmissibility and diagnostic escape, vaccination as an effective preventive strategy have been called to question. Interestingly, despite above mentioned challenges, efforts towards developing viable vaccine against Covid-19 intensified such that by November 2020, German company BIONTech in cooperation with United States company, Pfizer announced the successful development of their vaccine with 90% success rate and no side effect following clinical trials.13 It is known that 171 Covid-19 agents were tested in pre-clinical trials during development of Covid-19 vaccine and 64 Covid-19 agents’ vaccine are in clinical trials.14 These efforts culminated in eight vaccines developed and accepted for vaccination against Covid-19 under an emergency use authorization.15 With successful development and global vaccination campaign against Covid-19, studies have shown that vaccines against SARS-COV-2 have prevented infection and adverse outcomes for several SARS-COV-2 variant including Alpha and Beta variants.16 It was also revealed that two vaccines with either BNT 16262 or ChAd OX1 n Cov-19 as compared to no vaccine were independently associated with reduced PCR positivity in contacts. In furtherance, vaccination reduced transmission of SARS-COV-2 from vaccinated person who became infected by reducing viral load.17 With this revelation, there was massive deployment of vaccine against Covid-19 worldwide resulting in over eight billion doses of vaccines distributed as at November 21st 2021.18 In Nigeria four million doses of AstraZeneca/Oxford vaccine manufactured by serum institute of India was received by the Nigerian Government on 2nd March 2021. Rivers State started its campaign against Covid-19 on March 16, 2021 by vaccinating strategic leaders and frontline health care workers. In Bonny Island, vaccination commenced on 20th March 2021. The Covid-19 containment team deployed to Bonny by the State Ministry of Health were among the first set of frontline health care workers who received the vaccination, with the lead/corresponding author of this article who is the head of the containment team receiving the first Covid-19 vaccine in Bonny Island. The study objective was to ascertain the effectiveness of the AstraZeneca Covid-19 vaccine in preventing infection against SARS-COV-2 and its efficacy in preventing/reducing symptoms associated with the disease in infected persons. To the knowledge of the authors, there has not been any study of this kind in the state and more importantly Bonny Island, hence the study justification.
Material and methods
The study is a facility based cross-sectional study conducted at General Hospital Bonny, a Covid-19 testing, isolation and vaccination Center in Bonny Local Government Area of Rivers State Nigeria. Study population were respondents that have previously received Covid-19 vaccination who present to the facility for Covid-19 PCR test. With the use of formular for calculating sample size for cross sectional study, minimum sample size of 402 was derived, however 623 eligible respondents were included in the study. Exclusion criteria includes, respondents without verifiable proof of vaccination against Covid-19, participants with in-valid PCR test results and also individuals that declined participation in the study. Sampling technique involve enlisting all eligible respondents who presents to the facility from 6th may to 28th October 2021 for Covid-19 PCR test until sample size was achieved. A pretested adapted interviewer administered questionnaire prepared in English language was also used to collect information on socio-demographic profile and medical history including vaccination status and Covid-19 associated symptoms. Multinomial regression analysis using SPSS version 21.0 was used to analyze data with statistical significance set at 0.05. Results were presented in simple frequency distribution table. Ethical approval for the study was granted by the ethics review committee of River State Hospitals Management Board (RSHMB), permission for the study was also derived from the Chief Medical Director of RSHMB while informed consent was extracted from eligible respondents.
Results
Table 1. Socio-demographic profile
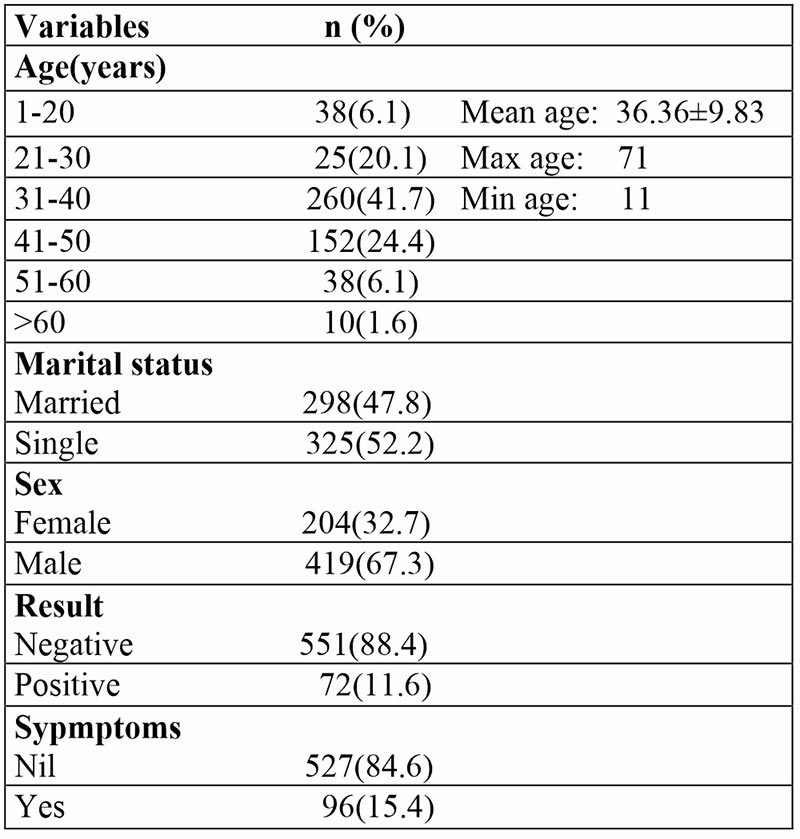
Most respondents were males 419 (67.3%) while age grade 31-40 were the most predominant 260 (41.7%) respondents.
Table 2: Multivariate regression analysis (vaccination status and socio-demographic profile)
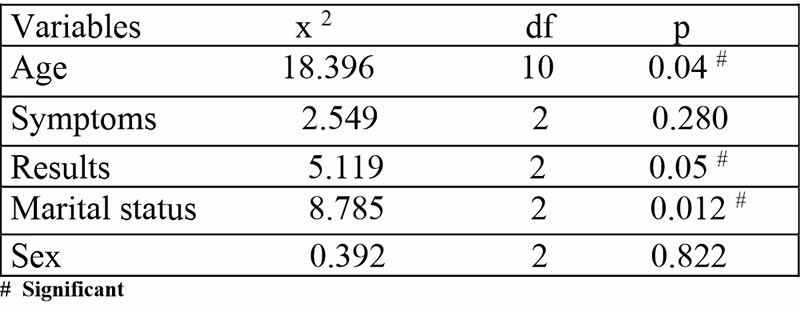
There was statistically significant association between Covid-19 vaccination status and age, marital status and Covid-19 PCR results.
Table 3: Univariate regression analysis (vaccination status and socio-demographic profile)
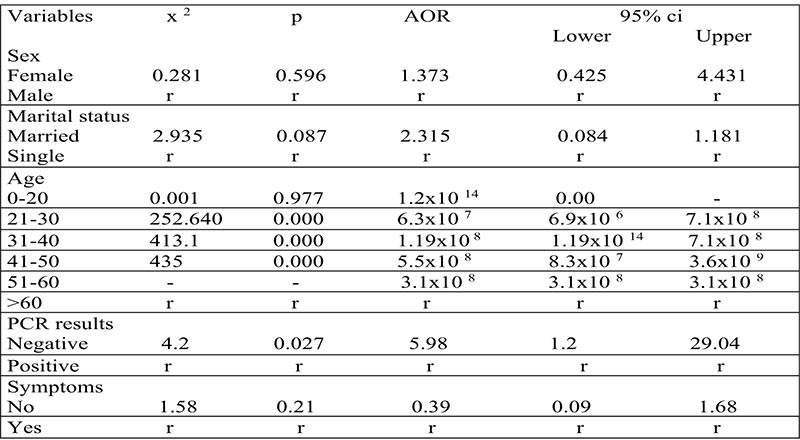
Age grade 0-20 and 21-30 years were the most and least responsive to vaccine uptake. Also, respondents who had received at least one dose of Covid-19 vaccine had 5.9 chances of a negative Covid-19 PCR test result compared to unvaccinated respondents.
Table 4: COVID-19 vaccination status and other variables
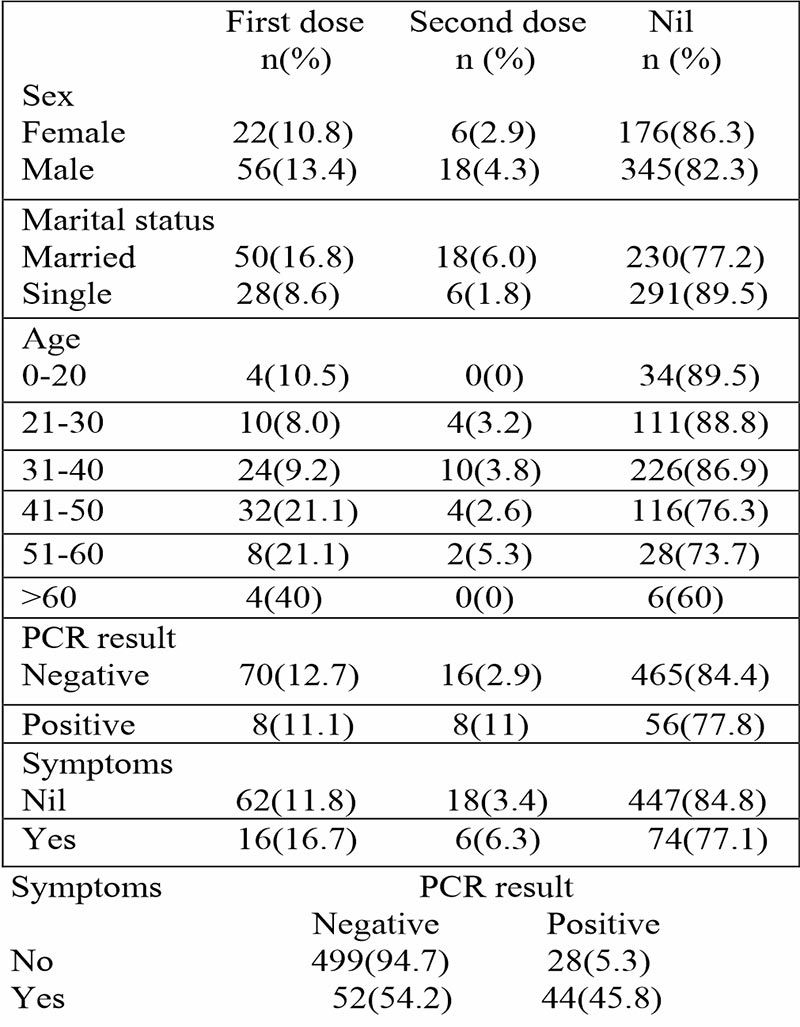
Most 521(83.6) respondents were hesitant to Covid-19 vaccination, while 52(54.2%) of respondents with negative Covid-19 PCR results claim to have symptoms of Covid-19.
Discussion
Findings from this study revealed statistically significant association between Covid-19 vaccination acceptance and age, marital status and result of Covid-19 PCR test results. As at the time of conducting this study, vaccine hesitancy was 83.6% among study respondents.
Covid-19 vaccine hesitancy in this study was high, this contrasts with most studies conducted in Nigeria in 2021 with lower vaccine hesitancy 41.8%19 and 50.5%.20 Study conducted in China reveals low vaccine hesitancy of 16.4%.21 Interestingly, most literatures reviewed were studies conducted in 2021 about same time with this study. Results obtained in this study were worrisome considering the study site was a Covid-19 testing and vaccination facility wherein sensitization and health education on Covid-19 was conducted daily before commencement of clinic. Also, respondents reside in Bonny town with access to health education via internet and other means of mass communication. It therefore reasons that people residing in the rural/remote communities of Bonny will have higher vaccine hesitancy rate due to poor education, geographic area, low socio-economic status and poor access to information which are known factors inhibiting vaccine acceptance.22 Also due to misperception and misinformation among residents derived mainly from myth associated with the vaccine which claims that the vaccine shortens life span, such misinformation and misperception have been shown to act as a significant barrier to achieving vaccine coverage and attainment of herd immunity.23 Such misperception could result from mistrust in viability of vaccine production as they were produced in a short period and approved under emergency use protocol. It requires about 10-15 years for vaccine development and production.24
Age was a significant predictor of vaccine acceptance in this study. Age grade 0-20 years had higher odds for vaccine acceptance while age grade 21-30 years the least. This result corroborates with results from similar studies which reveals significant association between vaccine acceptance and age.20,25 In contrast some studies found no significant relationship between age and Covid-19 vaccination.26,27 Interestingly and in conformity with our result, some studies identified age grade 20-29 with grater odds for vaccine hesitancy.20 There have been contrasting opinion among scholars over vaccine acceptance and hesitancy with age. Some authors submits that vaccine acceptance increases with age,28 while in conformity with our results, respondents of older age are less likely to accept vaccination.29 The age grade 0-20 years are most active with internet and computer use. They are most responsive to trending events including health issues. It is our belief that they would have fully enumerated the advantages inherent in vaccine uptake, and concluded to accept vaccination. Also, older persons present with more severe symptoms of Covid-19 than younger persons due to complications from co—morbidity common among older age grade, since vaccine introduced into the body cause an immune response like infection occurs naturally but there is no disease production.30
There was significant association found between marital status and Covid-19 vaccination. Results revealed higher odds for acceptance in favor of married couple. This result was also in tandem with result seen in other studies.31-33 Contrastingly, other studies disagree with our results.34,35 It is believed that married couples will engage and accept practices which protects their life and that of their family members. The anxiety to protect members of their family enhances the innate desire to conform to preventive practices.36,37
Respondents who are vaccinated against Covid-19 showed significant association with negative PCR test result. This result was in consonance with result from other studies.16,17 However, some authors have queried the protection provided against Covid-19 by vaccination. It was revealed that there was 76% protection from Covid-19 comparing Moderna vaccine and placebo.39 Also two vaccinations with either BNT16262 or ChAdox1n Cov-19 as compared to no vaccination were independently associated with reduced PCR positivity in contacts.17 It was additionally revealed that Covid-19 vaccination prevented infection and adverse outcomes for several SARS-COV-2 variant including Alpha and Beta variants.16 In furtherance, it was reported that viral load in a patient, is most likely associated with transmissibility of infection in contacts.40 It is believed that vaccination reduce the viral load thus preventing the transmission of the virus from an infected vaccinated person thereby reducing the risk of infection.17 This report is evidenced by a study which reveals that viral load observed in persons infected with a variant after vaccination are lower than those among unvaccinated persons.41
This study did not observe any significant association between vaccination against SARS-COV-2 and symptoms such as fever, cough, respiratory difficulty, loss of taste and smell sensation associated with the disease. Symptoms associated with the disease that was used. In divergence, report have shown 87% vaccine effectiveness against symptomatic Covid-19.10 It was also documented that vaccination prevented adverse outcome associated with Covid-19 and also reduced symptoms associated with the disease.16,17 However, it was suggested that protection against severe and symptomatic Covid-19 remains poorly understood.10 Most symptoms described by respondents in this study were not severe or life threatening and were similar to that of malaria, a systemic infection common in the tropics. Symptoms described by respondents were not exclusive to Covid-19 therefore, vaccination against Covid-19 could not have significantly moderated its effects. It is the belief of authors that the bizarre symptoms of Covid-19 which also obscure symptoms of malaria was indistinguishable to respondents. This is evidenced in the result which reveals 54.2% of respondents who tested negative to Covid-19 PCR test claim to have symptoms of the disease. Furthermore, subject bias whereby respondents claim not to have symptoms associated with Covid-19 apparently to maintain healthy medical records would have played a role in the results seen in this study. It is our belief that if these complicit factors are eliminated, there could be significant association between symptoms of Covid-19 and vaccination status.
There was no significant relationship between vaccination status and Gender. However, there was 1.37 odds in favor of female Gender for vaccine acceptance. Some studies also affirm that there was no significant association between vaccination status and Gender.20,33 In contradiction, few studies revealed significant association between gender and vaccination status with greater odds for acceptance in males than females.25,27 In consonance with our findings, some studies which did not establish significant association between Gender and vaccination status, however affirms higher odds for vaccine acceptance in females than males.20,42 Females are more conscious about personal health issues and less adventurist than males.36,37 This may give reason for greater vaccine acceptance in females.
Conclusion
There was significant statistical association between Covid-19 vaccination acceptance and age, marital status and result of Covid-19 PCR test result. There was no significant relationship between vaccination status and gender. This study was limited by its facility-based scope which rules out residents who do not believe in orthodox medicine. Our recommendation is to encourage a community-based study and also to enhance public enlightenment on the advantages of vaccination to improve on the vaccine acceptance rate.
References
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song j, Zhao X et-al. China novel Coronavirus investigating and research team. New England journal of Medicine 2020;382(8):727-733.
- Pragholapati A. Covid-19 impact on students. 2020; 10.17605/OSF.10/Nuhj9
- World Health Organization. Coronavirus disease 2019 (covid-19) situation report 46.2020.
- Olum R, Chekwech G, Wekha G, Nassozzi DR, Bongomin F. Coronavirus disease 2019: knowledge and practice towards Covid-19 among people living in Mosul-Iraq: a cross- sectional study. Plos one.2021;16(3): e0249310.10. 1371|journal.pone.0249310.
- Zhong BL, Luo W, Li Hm, Zhang QQ, Liu XH, Li WI et-al. Knowledge, attitude and practice towards Covid-19 among Chinese residents during the rapid period of Covid-19 outbreak. A quick online cross-sectional survey. Int.j.bio.sci.2020;16(10):1745-17521.
- Li R, Pei S, Chen B, Song Y, Zhang T, Yang W, Shaman J. Substantial undocumented infection facilitates the rapid dissemination of novel Coronavirus (SARS-COV-2). Science. 2020;358(6490):489-493.
- F-MJ. Soriano V. New SARS COV-2 variants challenge vaccines protection. Aids Rev.2021;2-3. 0.24875/ Aids Rev.m21000040.
- Kata A. Anti-vaccine activist, web 2.0 end the post of tactics and tropes used online by the anti-vaccination movement. Vaccine 2012;30(25): 3778-89.10.1016/vaccine. 2011.11.112.
- ReinKart R. Fewer in US continue to see vaccine as important. Gallup. 2020; 14:2020.
- Ssentongo P, Ssentongo AE, Voleti N, Groff D, Sun N et-al. SARS-COV-2 vaccine effectiveness against infection, symptomatic and severe Covid-19: a systematic review and meta-analysis. BMC infections disease. 2022;22(1):439.10.1186/s12879-022-07418-y.
- El-Shabasy RM, Yayel MA, Taher MM, Abdelmonem R, Shoueir KR, Kenawu ER. Three waves change, new variant strains and vaccination effect against Covid-19 pandemic. Int.j.biol.macromol 2022; 204:161-168.
- Aleem A, Samuel ABA, Slenker AK. Emerging variants of SARS-COV-2 and novel therapeutics against Coronavirus (covid-19). A preprint.
- WHO (2021) Coronavirus disease (Covid-19) pandemic. https://pubmed.ncbi.nih.gov/?term=who+(2021)+Coronavirus+disease+(Covid-19) pandemic
- Jia z, Hong W.Will mutation in the spike protein of SARS-COV-2 lead to the failure of Covid-19 vaccine. J Korean Med. Sci. 2021; 26:1-11. 10.3346/jkms.2021.36. E124.
- Klasse PJ, Nixon DF, More JP. Immunogenicity of clinically relevant SARS-COV-2 vaccines in non-human primates and Humans. Sci adv.2021,7: abe 8065.10.1126/sciadv. abe8065
- Lopez Bernal J, Andrews N, Gower C, Gallagher E, Simmons R, Theiwall S. et-al. Effectiveness of Covid-19 vaccine against the B.I.617.2 (delta) variant. N. England J med 2021;385;585-594. 10.1056/NEJMoa2108891.epub2021
- Eyre Dw, Taylor D, Purrer M, Chapman D, Fowler T, Pouwels KB, Walker AS, Peto TEA. Effect of Covid-19 vaccination on transmission of alpha and delta variants. N.Eng.J Med.2022; Nejmoa92116597 iv.1056/Nejmo92116597.
- Mathieu E, Ritchie H, Ortiz-Ospina E, Roser M, Hassel J, Appel C, Giattino C, Rodes-Guirao L. A global database of Covid-19 vaccination. Nat human behave. 2021; 27:1-7.
- Oluwatemitope OC, Kehinde SV, Felicia UB, Olabisi OA, Eziachi AE, Martin IC et al. Predictors of uptake of a potential Covid-19 vaccine among Nigerian adults. MedRxiv.2021;1-2
- Amuzie CI, Odini F, Kalu KU, Izuka M, Nwamoh U, Ukaegbu UE, Onyike G. Covid-19 vaccine hesitancy among health care workers and its socio-demographic determinants in Abia State, South Eastern Nigeria: across sectional study. Pan African Med. J. 2021;40.10.10.11604/pamj.2021.40.10.29816
- Lin Y, Hu Z, Zhao Q, Alias H, Dangee M, Wong LP. Understanding Covid-19 vaccine demand and hesitancy: a nationwide online survey in China. Plos negl trop disease. 2020;14(12): e0008961
- Galarce EM, Minsky S, Viswanath K. Socio-economic status, demographics, beliefs and A (HiNi) vaccine uptake in US. Vaccine. 2011;29(32): 5284-89.10.1016/j.vaccine.2011.05.014
- Lane S, Mac Donald NE, Marti M, Dumolard L. Vaccine hesitancy around the globe: analysis of three years of WHO/UNICEF joint reporting form data 2015-2017. Vaccine 2018;36(26):3861-67.10.1016/j vaccine.2018.03.063
- Sharma O, Sultan AA, Ding H, Triggle CR. A review of the progress and challenges of developing a vaccine for Covid-19. Front Immuno.2020;11:585354
- Yahia AID, Alshahrani Am, Alsulmi WGH, Algarni MMM, Abdulrahim TKA et al. Determinants of Covid-19 vaccine acceptance and hesitancy: a cross sectional study in Saudi Arabia. Hum vaccin immunother. 2021;17(11):4015-4020.10.1080/21645515.2021.1950506
- Al- Mohaithef M, Padhi BK, Ennaceur S. Socio-demographic correlates of Covid-19 vaccine hesitancy during the second wave of Covid-19 pandemic: a Cross sectional web-based survey in Saudi Arabia. Frontier in public health. 2021; 9:698106.10.3389/fpubh.2021.698106.
- Okmi EA, Almohammadi E, Alaamri O, Alfawaz R, Alomari N et al. Determinants of Covid-19 vaccine acceptance among the general adult population in Saudi Arabia based on the health belief model. A web based cross sectional study. Cureus 2022;14(8): e28326. 10.77159/cereus.28326
- Biswas N, Mustapha T, Klubchandani J, Price JH. The nature and extend of Covid-19 vaccination hesitancy in health care workers. J comm health. 2021;1-8
- El- Elimat T, Abu Alsamen MM, Alali FQ. Acceptance and attitudes towards Covid-19 vaccines: a cross sectional study from Jordan. Plos one. 2021;16(4): e0250555
- Calina D, Sarkar C, Arsene AL, Slehi B, Docea AD, Mondal M, Islam MT, Zali, Sharifi-Rad J. Recent advances, approaches and challenges in targeting pathways for potential Covid-19 vaccine development. Immuno. Res. 2020;68(6):315-324. 10.1007/s12026-020-09154-4
- Wang J, Jing R, Lai X, Zhang H, Lyu Y, Knoil MD et al. Acceptance of Covid-19 vaccination during the Covid-19 vaccination during the Covid-19 pandemic in China. Vaccine (Basel) 2020;8(3):482
- Padhi BK, Al- Mohaithef M. Determinants of Covid-19 vaccine acceptance in Saudi Arabia: a web based national survey. J Multidiscip health care. 2020; 13:1657-1663
- Al-Mohaithef M, Padhi BK, Ennaceur S. Socio-demographic correlates of Covid-19 vaccine hesitancy during the second wave of Covid-19 pandemic: a cross section web-based survey in Saudi Arabia. Frontiers in public health. 2021; 9:698106.10.3389/fpubh.2021.698106
- Ai M, Hossain A. What is the extent of Covid-19 vaccine hesitancy in Bangladesh: a cross sectional rapid national survey. BMD. Open 2021;11(8)e050303
- Kasrine Alhalabi C, Obeid S, Sacre H, Akel M, Hallit R, Salameh P. et al. Attitudes of Lebanese adults regarding Covid-19 vaccination. BMC public health. 2020;21(1):998
- Ogbondah BO, Owhonda G, Luke A, Jaja I, Green P, Pius OM. Covid-19: Determinants and Barriers to infection prevention and control practice among residents in Bonny Island, Rivers State. The Nigerian Health Journal. 2022;22(4):371-381
- Ogbondah OB, Owhonda G, Jaja I, Luke A, Pius OM. Covid-19: socio-demographic determinants of knowledge. Ibom Medical Journal. 2022; 15(3) 22:236-244
- Lumley SF, O’Donnel D, Stoesser NE, Mathews PC, Howarth A, Hatch SB et al. Antibody status and incidence of SARS-COV-2 infection in health care workers. New England Journal of Medicine. 2021;533-540. 10.1056/NEJMoa2034545
- Baden LR, El Sally HM, Essink B, Kotloff K, Frey S et al. Efficacy and safety of the mRNA-1273 SARS-COV-2 vaccine. New England Journal of Medicine. 2021; 384:403-416. 10.1056/nejmoa2035389
- Marks M, Millat-Martinez P, Ouchi D, Roberts CH, Alemany A, Ubals M. et al. Transmission of Covid-19 in 282 clusters in Catalonia Spain: a cohort study. Lancet Infect Disease. 2021; 21:629-636
- Levine-Tiefenbrum M, Yelin I, Katz R, Herzel E, Golan Z, schreber L, Wolf T. et al. Initial report of decreased SARS-COV-2 viral load after inoculation with BNT162b2 vaccine. Nat Med. 2021; 27:790-792